
Virus
To “debris” or not to “debris,” that is the question.


It was inevitable that we would get to this question.
Are there viruses?
If I reflect on my journey with this question, my answers have progressed along the following lines:
Why would you even ask such a stupid question?
To…Most definitely.
To…Yes.
To…I don’t know, plus I don’t quite know how to think about the question.
To…They have lied to me about everything else, so what are the chances everything in this virus space is true? Zero.
To…I don’t know what is and is not true in the virus space…so I’m still searching for help on how to think about the question and then answer it with confidence.
So, that is where I’m at. I’m very curious and very open to build a new framework of understanding around the whole “virology thing.”
My gut feel says, they have lied to me about it.
My gut feel also says there is likely a form of “information communication” between one person to the next. Are those information “packets,” assuming they exist, what they are calling “viruses”?
I’ve been looking for two things to help me get closer to some answers.
A highly credible person. For me, ideally that means I’ve been able to consider their truthiness and the quality of their thinking in a different domain.
That person then helps me to understand and consider some original, primary, source information and data.
I believe I have done that with Dr. Thomas Cowan and his book Breaking the Spell.
For those that don’t know Cowan, I would strongly recommend:
Vaccines, Autoimmunity, and... by Cowan MD, Dr. Thomas (amazon.com)
It’s not a long book, but it’s an absolute gem.
Cowan is a big deal for many people, and he’s a big deal for me. A good and courageous man, who knows a lot about a lot. So that’s a good start. It doesn’t automatically mean that he’s right about viruses, but it’s a damn good starting point.
I strongly recommend you read his short book called Breaking the Spell.
What I’m going to focus on are the first two, fairly short, chapters, where he explains virology to us, its past and present.
If anyone can directly falsify, with evidence, any point that he makes below, I definitely would like to hear it.
As I said, I don’t know whether Cowan is right, but he has earned the right to be given the benefit of the doubt on this question and to be heard.
I will add some thoughts and comments as we go through the two chapters.
With thanks and appreciation to Dr. Thomas Cowan.
All emphasis added is mine.
Breaking the Spell: The Scientific Evidence for Ending the Covid Delusion.
Chapter One
HOW DOES A VIROLOGIST IDENTIFY THE EXISTENCE OF A NEW VIRUS AND PROVE THAT IT CAUSES DISEASE?
No one would hire a baker who couldn’t describe the exact steps he or she would use to bake a cake. Similarly, no one would hire a carpenter to build a woodshed who had never heard of a hammer. And any person who doesn’t know the exact steps a virologist takes to answer the question posed in the title of this chapter can’t possibly judge whether SARS-CoV-2, the virus that allegedly causes COVID-19, exists.
To be clear, I don’t mean an answer such as, “you do a test for the virus,” or, “all doctors believe there is such a virus.” I am specifically referring to the steps any virologist in the world should take to identify a new virus. I am convinced that once you understand exactly these steps, you will never again believe that any virus has ever caused any disease. As hard as it might be to accept, the truth is that simple.
In a sane and rational world, medical authorities would have made the answer to this straightforward question the first and highest priority in their role as educators of the population. As you will see, the process is simple to understand. Thus, there is no reason every person in the world should not know how to answer this basic question.
As my experience during the past year of giving hundreds of talks, lectures and interviews has taught me, however, almost no lay person, journalist, lawyer, activist or health professional, including MDs, has any idea how to answer this question. For many, COVID has become their life’s work, yet they still have no idea how to even know whether this virus exists. After you read the next 10 pages or so, I am hopeful that you, unlike these professionals, will never again be in this predicament.
First, let’s start with how the overwhelming majority of lay people and health professionals alike believe that a virologist goes about proving the existence of a virus.
When I have asked people this question, the answer I most often hear is, “Millions of people all over the world are getting sick and dying; therefore, it must be a virus.” Often, people claim that it has been shown that the disease has spread from place to place, or from person to person, which must “prove” that the cause is a virus. Sometimes, they point to stories they have read, such as, “San Quentin prison had no cases of COVID, and then someone with COVID was sent there, at which time many people got sick” (or at least tested “positive”), which again proves it must be a virus.
Sometimes, it is the story of Aunt Bessie, who went to church, only to fall ill a week later after having been exposed to someone at church who tested positive. I have heard scores of such stories. The important point to make is that no scientist, virologist or competent medical professional would claim that these epidemiological observations prove the existence of any virus. In fact, the role of epidemiology in medicine and science is primarily to generate hypotheses, which then can be tested in the laboratory to prove causation. Epidemiology can never prove the existence of any virus, nor prove the cause of any disease.
That is simply not its role. On this, there is virtually no disagreement in the scientific world.
Furthermore, if the fact that a lot of people getting sick in the same place proves viral causation, then we could logically conclude that Hiroshima must have been a virus. If we claim that a disease that spreads is also proof of viral causation, then the Chernobyl disaster could have been caused by a virus.
This unfortunately is a rhetorical strawman, and I would have preferred Cowan didn’t use such a weak argument.
For more than a hundred years, people observed that one sailor after another got sick on ships. Their teeth fell out, and many went into heart failure and died. For many, it was “obvious” that something was being passed—a contagion—from one sailor to the next. At some point, however, a sailor ate a lime; the whole thing went away because, in fact, the sick sailors were suffering from scurvy, a disease caused by vitamin C deficiency.
This is a much stronger point in my opinion. Understanding disease and bad health through a “deficiency” framework. There is a long list of conditions that were thought to be “caused by something external” only to discover decades or even centuries later that it was an internal deficiency that prevented good health.
There are many other examples illustrating how epidemiological observations have misled a medical profession stubbornly wedded to the idea of contagion. Beriberi and pellagra, two well-known nutritional deficiencies, were considered for decades to be caused by a contagion. It turns out the cause was B vitamin deficiency, which, as one would expect, would often show up in the same family members at the same time.
This is the main point that I need help with. The question of contagion.
Is there such a thing? Obviously, Cowan doesn’t believe in contagion, but it’s not a question addressed in this short book.
To reiterate the point, the role of epidemiology in science is—or should be—to suggest avenues to explore. And when scientists misuse epidemiology, they become, in the words of the former chair of Harvard’s epidemiology department, “a nuisance to society,” doing “more harm than good”1.
In the case of “COVID,” I have no objection to exploring the hypothesis that some infectious agent is the cause of this potentially new illness, but I also contend that many other possible causes should be explored. To be even clearer, using epidemiology to prove this or any virus exists is a scientifically naive and irrational stance.
Let’s take the next step. Here, we are describing what most people think has happened and what the vast majority of medical doctors believe has happened. Most people assume that the first thing researchers do when confronted with a new illness is carefully define the symptoms. Then, once they have found a significant number of similarly sick people, the assumption is that the researchers examine various bodily fluids from the sick people to find a common virus. The general expectation is that the virus will then prove to be abundant in these people, that it will demonstrate a uniform morphology (size, shape and other defining physical features) and that each virus (called a virion) will be shown to contain the identical genetic material. This is the clear, logical and rational approach to the discovery of a new virus.
The actual facts contradict this rational approach. Although some “viral” diseases do share a common symptom picture, many, such as “COVID-19,” do not. This phenomenon obviously complicates matters, for without a clear definition of the illness as a starting point, identifying which sick people to examine immediately becomes a challenging hurdle. But even in the most clearly defined “viral” diseases, such as measles or chicken pox, the following shocking statement is still undeniably true: In the history of medicine, not one published study shows the isolation of identical particles that would represent a disease-causing virus from any bodily fluid from any sick person.
Let me make this even more clear. If one takes any person with any “viral” illness—for example, chicken pox, rabies, measles, AIDS or COVID-19—the published literature does not contain any evidence of any virus that was directly isolated from any bodily fluids from even one person suffering from these illnesses. The interesting thing about this statement is that no health institution from any government in the world disagrees. Similarly, there is no disagreement on this point from any virologist or medical doctor who works in or publishes in the field of virology. And there is no disagreement about this statement from such institutions as the Centers for Disease Control and Prevention (CDC), the Pasteur Institute or the Robert Koch Institute.
This is a stunning passage in italics.
It has the potential to be on par with the realization that there is not a single vaccine that has been tested against a true placebo.
In fact, the ramifications of this passage are even greater.
To prove this point, we are in possession of nearly 60 written statements from governmental institutions from all over the world confirming that they have no examples of SARS-CoV-2 being isolated directly from any human being2. We also have written statements from some of the lead authors of the most important papers on the “isolation and purification” of SARS-CoV-2, who agree that they never attempted to obtain the virus directly from any fluid of any sick person3. Finally, in-person communication with a number of virologists confirms that no pathogenic virus can be isolated from any bodily fluid of any sick person. They simply say that is not the way the science is done.
Let’s be very clear, though, on the next point. It isn’t that it is technically impossible, or even difficult, to isolate any particle the size and shape or characteristic of a virus from a fluid sample. For decades, for example, scientists have isolated identical particles (called bacteriophages) from bacterial cultures and showed pure samples of these particles under the electron microscope. In this case, all particles from one culture are morphologically identical, all are made of exactly the same proteins, and all have identical genetic sequences.
The steps to isolate a particle the size and characteristic of a virus are also straightforward and not unlike how a chemist would isolate caffeine from a coffee bean. First, you take a sample of whatever fluid you wish to examine. Then, you macerate it (as in a blender) and filter the sample through a filter paper that allows anything soluble, including any particle the size of a virus, to pass through the paper. After discarding the cells, fungi and bacteria, you put the remaining fluid on something called a “sucrose density gradient,” which separates it into bands by molecular weight. This process is called ultracentrifugation.
With ultracentrifugation, the virus in question spins out into a band. The band can then be extracted from the gradient with a micro-pipette and checked for purity. In this way, you can confirm that the only thing in the band is the virus. You can then study the virus, determine its exact morphology and sequence its entire genome. Most importantly, you can then expose test animals to this isolated, purified virus to see whether they get sick.
These steps are the way science is supposed to work. One isolates the variable—in this case, the virus—and then characterizes the make- up of the virus. Once one is certain of the existence of the pure virus, test animals can be exposed to it. Yet this simple, doable experiment has never been successfully done for even one so-called viral disease, and it has certainly never been attempted for COVID-19 and SARS- CoV-2. Not even once.
When I ask doctors or virologists why they don’t carry out this simple, clear, logical, rational proof to demonstrate the existence of a new virus and show it causes disease, I hear one of two answers. The first is that not enough of the virus is present in any bodily fluid of any sick person to find it in this way. I have even asked scientists whether they would see the virus if the bronchial fluid from 10,000 people with “COVID” were pooled, but the response is the same: “There is not enough virus to find.” This, of course, begs the question: On what theory are we then claiming the virus is making people sick? To this, there is no answer.
I think Cowan is making a fair point here.
But we are left with the question of whether anyone was sick with covid during covid.
My answer is Yes.
It was not the flu, and it was not a cold. People got sick, and it was something else. Personally, I had covid for about 3 days and then was left with a 6-week cough that seemed like it would never go away. It wasn’t my imagination. Obviously, there were millions around the world who came down with something. The question is, what was it?
Which brings me to the subject of “infectious clones” something JJ Couey gets all the credit for introducing into the dissident vernacular.
I don’t know what Cowan would say about Infectious Clones, but they need to be reconciled with Cowan’s work, in my mind.
The second answer I have heard is that viruses are intracellular “parasites”—so, of course, we can’t find them outside the cells. When asked how the virus passes from one person to another, as we are told it does, virologists reply, “it buds out of the cell, goes into a droplet and travels to the next person.” In other words, the virus is transmitted when it is outside of the cell. I can only wonder why virologists can’t find it during this transmission step since they clearly think it is outside the cell.
We are faced here with a dilemma. It is clear that no virologist has ever isolated any pathogenic virus from any bodily fluid of any sick person. How, then, can virologists claim—in thousands of papers, including scores on SARS-CoV-2 alone—that a virus was “isolated,” characterized and shown to cause illness in animals? There are hundreds of claims that the genome of SARS-CoV-2 has been sequenced, and that variants of this genome have been discovered. Understanding how virologists have felt justified in making this claim is the key to understanding how virology lost its scientific integrity.
If they are not following the straightforward steps I have described for isolating a virus, on what basis do virologists claim the existence of a new virus and the proof that this new virus is a pathogen? The answer is simple: Virologists claim that something called the “cytopathic effect” is the proof of the existence of a virus and its disease-causing potential. Again, about this statement there is no dispute.
To understand what cytopathic effect is, we must revisit some pivotal events in the history of virology that occurred in the early 1950s. Around that time, virologists realized that they had the tools to see particles the size and morphology of a virus using the electron microscope; however, they also realized that they never saw a uniform particle coming from any sick person. In essence, they disproved the foundation of virology!
Fortunately for the virology profession, a man named John Franklin Enders saved the day by “discovering” the process that became known as the viral “culture,” a discovery for which he received a Nobel Prize in 1954. In 19544 and 19575, Enders wrote two papers describing how to create viral cultures (using a “minimal nutrient medium”), and this methodology became the standard for all viral proofs forevermore.
Remember, a virus is an extremely small particle, one that can be seen only with the magnification available through an electron microscope. Also remember that a virus is conceived to be a tiny particle with a protein coating encasing a small amount of genetic material, either DNA or RNA. The game is to find this unique particle and show that it causes destruction of the host on which it grows.
Bearing these aspects of the definition of a virus in mind, here are the steps Enders outlined in his 1954 paper (4). Enders started his experiment by taking a throat swab from seven children hospitalized with symptoms consistent with measles. He mixed the cotton swab with two milliliters of milk—interestingly, itself a source of genetic material. Then he added the throat swab in milk to a solution containing:
“Penicillin, 100ug/ml and streptomycin, 50 mg/ml were added to all throat specimens which were then centrifuged at 5450 rpm for about one hour. Supernatant fluid and sediment resuspended in a small volume of milk were used as separate inocula in different experiments in amounts varying from 0.5 ml to 3.0 ml” (4).
“Inocula” is just the sample used in the next step, which was to inoculate this material onto a culture of “trypsinized human and rhesus monkey kidney” cells. To this culture medium, he added the following:
“The culture medium consisted of bovine amniotic fluid (90%), beef embryo extract (5%), horse serum (5%), antibiotics, and phenol red as an indicator of cell metabolism” (4).
In simple language, Enders mixed his sample with six other sub- stances that are known to be sources of protein and genetic material. We now know that these substances break down into particles with the size and morphology of what are called viruses. These six sources are milk, human kidney cells, rhesus monkey kidney cells, bovine amniotic fluid, beef embryo extract and horse serum.
To this culture, Enders’ research group next added antibiotics that are known to be toxic to the kidney cells, especially streptomycin. (Nowadays, scientists tend to use the antibiotics gentamicin and amphotericin.) Enders and colleagues then observed this brew over a number of days. When they saw a characteristic cytopathic effect (CPE) in the cells of the cultures—meaning the transition of healthy, normal-sized culture cells into giant, disorganized cells with internal holes or vacuoles—they concluded that these were proof that the virus from the throat swab was destroying the cells in the culture. To Enders, this cytopathic effect was the hallmark of dying cells, and he believed it could only have occurred because the virus in the measles sample infected and destroyed the cells in the culture.
This is such an incredible passage.
All I can say is…What the hell is going on!!??
If you were explaining this to a 6-year old kid, it would go something like this:
Imagine you have tiny building blocks that are healthy and neat. Enders and his friends added some special liquid to these blocks. Then, they saw the blocks become really big and messy with holes in them, kind of like a cheese with holes. They said that this happened because a tiny, tiny bug from someone's throat got into the blocks and started causing trouble, making them change and look funny.
To this day, with minor exceptions, every “viral isolation” starts with this flawed culturing process. Furthermore, every genetic analysis of any purported virus is done on the results of this cell culture, not on an isolated, purified virus. No exceptions. Thus, if virologists want to elucidate the genome of a new virus, they don’t isolate the virus from a sick person and sequence that specific particle. Rather, they take an unpurified sample from a sick person, run it through a tissue culture (as described above) and do their analysis on the resulting mixture—not on the virus itself.
Once one understands how this process works, it gives rise to two central questions. First and foremost, how can we be sure—absolutely sure—that the CPE is a result of a virus from the sick person and not the result of a cell culture that is starved and poisoned? Second, how can we be certain—absolutely certain—that any resultant particles and genetic material in the final culture came only from the growth of the virus from the sick person and not from one of the six substances added to the culture that are also known to contain proteins, “viruses” and genetic material? These two questions are at the foundation of the entire edifice of virology, but astonishingly, the rigorous controls that might provide answers are never done.
Interestingly, Enders himself was aware of the potential pitfalls of his experimental method, for he pointed out the following:
“A second agent was obtained from an uninoculated culture of monkey kidney cells. The cytopathic changes it induced in the unstained preparations could not be distinguished with confidence from the viruses obtained from measles.” (4).
In other words, although Enders didn’t describe his control experiment in detail, he did tell us that he repeated this entire cell-culture experiment, but this time he added nothing from any sick person. The CPE and the resultant particles he obtained “could not be distinguished” from the results he obtained when he inoculated the culture with measles. This is strong evidence that any CPEs were caused by the culture conditions, not by any alleged virus coming from the measles patients.
Again, if you were explaining all this to a child, it would go something like this:
Enders, a scientist, found that when he did an experiment with kidney cells without adding anything from sick people, the cells still changed in a way that looked just like when he did use stuff from sick people, suggesting the changes might be caused by the experiment itself, not the sickness.
In Enders’ follow-up paper in 1957, he repeated his concerns about his experimental method. He started by stating:
“Ruckle has lately reported similar findings and in addition has isolated an agent from monkey kidney tissue that so far is indistinguishable from human measles virus.” (5).
In other words, a second virologist, Ruckle, found particles coming from monkey kidney cells that, again, were “indistinguishable” from what Enders called the human measles virus.
An important-to-understand corollary of Enders’ precedent-setting “discoveries”—and something that almost no physician or lay person realizes—is that every “live-viral vaccine” basically is nothing more than a partly purified (minimally filtered) cell culture mixture. Measles vaccination programs involve the injection of the results of this cell culture experiment on a large scale.
Ok, I now want to vomit.
So, are you telling me that the whole idea of injecting a “dead or harmless virus” as part of vaccination is ALSO a sham.
When in fact they are injecting “cell culture mixture”…
Honestly…I have run out of words to describe the madness and insanity in this space.
Later in the 1957 article, Enders reiterated the central dilemma: How can we know the origin of the particles that he chose to call the human measles virus? In this particular quote, he referred to the problem in the context of vaccines:
“There is a potential risk in employing cultures of primate cells for the production of vaccines composed of attenuated virus, since the presence of other agents possibly latent in primate tissues cannot be definitely excluded by any known method” (5).
What is clear from the work of Enders is that he had no idea whether the origin of the particles he claimed were the human measles virus actually came from the sick person or were the result of the breakdown of one of the sources of genetic material used in the cell culture.
In the 1950s, there was no way to distinguish an exogenous, pathogenic virus from the normal particles formed when dying cells break down. Surely, 67 years later, with our modern analytical tools, virologists must be able to distinguish between these two entities. However, here is what a May 2020 paper concerning exactly this issue had to say:
“The remarkable resemblance between EVs [extracellular vesicles] and viruses has caused quite a few problems in the studies focused on the analysis of EVs released during viral infections…. However, to date, a reliable method that can actually guarantee a complete separation does not exist”6.
Today, virologists refer to the inevitable breakdown products of dead and dying tissues as extracellular vesicles or sometimes as “exosomes.” These particles can be isolated and purified directly from bodily fluids of sick people. They are conceptually different from viruses in that viruses supposedly come from outside the person and, at least sometimes, are considered pathogens. EVs come from the breakdown of the person’s own tissues and are non-pathogenic. And, as of May 2020, virologists acknowledged that they can’t distinguish between the two (6).
To anyone that knows the answer…is the word “virus” as here explained by Cowan interchangeable with “exosome”?
There is only one realistic explanation for this. All particles with the size, composition and morphology of “viruses” are, in reality, the normal and inevitable results of the breakdown of our own tissues. And our tissues break down for the same reason as the cultures in Enders’ experiments broke down: They’re either starved, poisoned or both.
Dying tissues produce a myriad of particles, and these particles have unfortunately been mistaken for pathogenic, exogenous viruses. It’s time to clear up this misconception.
Chapter Two
MODERN “ISOLATION” OF SARS-COV-2
It is instructive to examine carefully one of the most influential papers written about the isolation and characterization of SARS-CoV-27. The importance of this paper is that it claims to document the isolation of SARS-CoV-2 from the first patient diagnosed with COVID-19 in Australia. Therefore, it takes its place as one of the most critical papers published regarding the emergence of SARS-CoV-2 outside of its sup- posed country of origin, China.
As you will see, the authors of this paper (Caly et al.) follow the same script as the one used by Enders more than six decades ago. In the first section, they describe the clinical situation of the affected patient. Then comes the hunt for the virus. As always:
“Material from the initial nasopharyngeal swab was used to inoculate a Vero/hSLAM cell line” (1).
Translated, this means that an unpurified sample of the mucus from the patient’s nose and throat was inoculated onto a culture of monkey kidney cells. The researchers made no attempt to look for the actual virus or to test for the genome of the virus in the swab sample from the patient. Only a RT-PCR (reverse transcription polymerase chain reaction) analysis was done, which I will discuss in the next chapter.
In the body of the paper, there is no description of the actual culture methods, but in the supporting material, the authors describe the usual use of a minimal nutrient medium and the addition of two antibiotics (gentamicin and amphotericin) to the growth medium. Predictably, this starvation and poisoning of the cells results in the cells’ breaking down (the CPE) and the production of “viral” particles liberated into the culture medium. This process also means that, along with extracellular vesicles/viruses, numerous sources of genetic material will be present in the final culture. These include any potential exogenous viruses that might have infected the patient (if such viruses even exist), genetic particles from the unpurified swab sample from the patient, fetal calf serum and the monkey kidney cells. Yet Caly and colleagues make no attempt to determine where the genetic material that was test- ed for originated.
The authors then describe the electron micrographs done on the resulting culture fluid:
“Electron micrographs of sectioned Vero/hSLAM cells showed cytoplasmic membrane-bound vesicles containing coronavirus particles (Box 5, B). Following several failures to recover virions with the characteristic fringe of surface spike proteins, it was found that adding trypsin to the cell culture medium immediately improved virion morphology” (1).
In other words, the particles the Australian researchers call “coronaviruses” included the characteristic halo of spike proteins only after the investigators added trypsin to the culture medium. Trypsin is a protein-digesting enzyme; viruses are alleged to have a protein “coat.” It would be reasonable to assume that if one adds protein-digesting enzymes to particles with a protein coating, some of the protein coating will be eaten away, leaving a final particle that might look in an electron micrograph as if it has spikes. This lab-induced result obviously would bear no relationship to what such a particle might look like inside a live person.
There is only one rational, logical and scientific conclusion that one can draw from this paper: These researchers had no idea what made the Vero/hSLAM cells break down. Moreover, they had no idea where any genetic material they subsequently tested for originated. Finally, they did not find any particle with the characteristic morphology of a coronavirus until they manufactured its appearance. In sum, there is no evidence in this paper that any particle known as SARS-CoV-2 was found, or that any virus had anything to do with this Australian person’s illness.
In every paper published on the “isolation” and characterization of SARS-CoV-2, the first step in the experiment is to do the viral culture. Every analysis of the genome of the “virus” has been done on the results of these culture experiments, not on fluid taken directly from any sick person. Conventional virologists present the CPE (cytopathic effect) as THE proof that the virus exists AND causes disease.
Thus, our next step is to look at the recent experiments of Stefan Lanka as he attempted to do proper scientific studies to understand exactly how the CPEs that virologists are reporting come about8. Stefan Lanka, a virologist who is credited with discovering the first “giant” virus living in an organism in the ocean, decided to put the cy- topathic-effect phenomenon to a rigorous test. The question he tried to answer is a simple one: Is the CPE caused by the presence of a patho- genic virus, or is it the result of the culturing process?
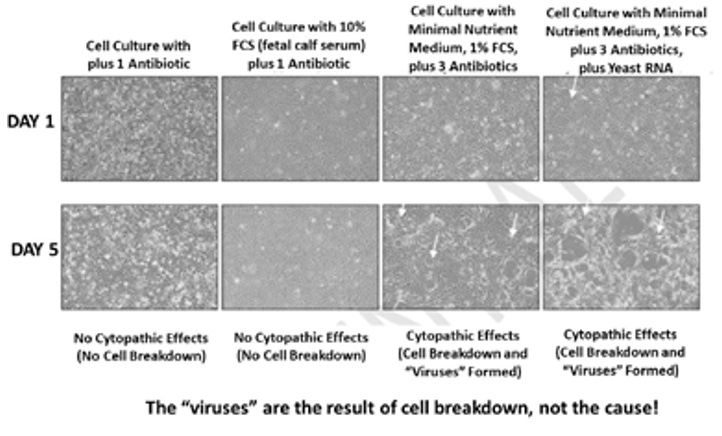
Here is the essence of Lanka’s experiment, done by an independent professional laboratory that specializes in cell culturing. As seen in this series of photographs, each of the four vertical columns is a separate experiment. The top photo in each column was taken on day one, and the bottom photo was taken on day five.
In vertical column one, normal cells were cultured with normal nutrient medium and only a small amount of antibiotics. As you can see, on neither day one nor day five was any CPE found; the cells continued their normal, healthy growth.
In vertical column two, normal cells were again grown on normal nutrient medium and a small amount of antibiotics, but this time, 10% fetal calf serum was added to enrich the medium. Still, the cells in the culture grew normally, both on day one and day five.
The third vertical column shows what happened when Dr. Lanka’s group used the same procedures that have been used in every modern isolation experiment of every pathogenic virus that I have seen. This included changing the nutrient medium to “minimal nutrient medium”—meaning lowering the percentage of fetal calf serum from the usual 10% to 1%, which lowers the nutrients available for the cells to grow, thereby stressing them—and tripling the antibiotic concentration. As you can see, on day five of the experiment, the characteristic CPE occurred, “proving” the existence and pathogenicity of the virus—except, at no point was a pathogenic virus added to the culture. This outcome can only mean that the CPE was a result of the way the culture experiment was done and not from any virus.
The fourth and final vertical column is the same as vertical column three, except that to this culture, a solution of pure RNA from yeast was added. This produced the same result as column three, again proving that it is the culture technique—and not a virus—that is causing the CPE.
The reason for adding the yeast RNA is because of the way that the genome of a “virus” is found, a computerized process called “alignment.” The alignment process starts with fragments of RNA and constructs a theoretical genome—one that never exists at any point in the actual sample. This genome never exists in any person, and it never exists intact even in the culture results; it exists only inside the computer, based on an alignment process that arranges these short pieces into an entire “genome.” It is for this reason that every complete genome of SARS-CoV-2 is referred to as an “in silico” genome, meaning a genome that exists only in the computer. As long as you have enough of these RNA fragments and provide the template, the computer can recreate any genome.
I need someone to try to disprove and falsify Cowan here.
He is either right or wrong and I really would like this point triangulated.
If he is right, what does that mean?
What did the PCRs ping positive for?
Did the PCRs also ping for infectious clones or where they a different genome and “invisible” to the PCR?
Knowing how the alignment process works, we can now understand what Dr. Lanka’s fourth experiment actually showed. He was able to show that any RNA virus genome can be found in the results of the cell culture from the fourth experiment. Yet at no time were any of these viruses added or present in the experiment.
At this point, it should be clear that the existence of SARS-CoV-2 has never been scientifically proven. And because the virus has never been shown to exist, there is no way we can conclude that this virus causes any disease, has any “variants,” contains any particular protein—in particular, the now famous spike protein—or has any other characteristics.
In addition, we can now turn our attention to the COVID tests. If the virus hasn’t been shown to exist, and if the main researchers who came up with the tests for the virus admit in writing that they never worked with or had possession of an actual virus9, what, actually, is a COVID test looking for? This question also points to an important corollary, which is to understand how COVID testing has been manipulated to implement governmental measures that have done great harm to the peoples of the world.
Thanks for being here.
Please consider a paid subscription.
You will get nothing more for your support, as everything is made freely available. The money goes towards covering the costs of this work, medical freedom causes and support for the vaccine injured.
I am always looking for good, personal GMC, covid and childhood vaccination stories. You can write to me privately: unbekoming@outlook.com
If you are Covid vaccine injured, consider the FLCCC Post-Vaccine Treatment
If you want to understand and “see” what baseline human health looks like, watch (and share) this 21 minutes
If you want to help someone, give them a book. Official Stories by Liam Scheff. Point them to a “safe” chapter (here and here), and they will find their way to vaccination.
Here are all eBooks and Summaries produced so far:
FREE Book Summary: The HPV Vaccine on Trial by Holland et al.
FREE Book Summary: Bitten by Kris Newby (Lyme Disease)
FREE Book Summary: The Great Cholesterol Con by Dr Malcolm Kendrick
FREE Book Summary: Propaganda by Edward Bernays
FREE Book Summary: Toxic Legacy by Stephanie Seneff (Glyphosate)
FREE Book Summary: The Measles Book by CHD
FREE Book Summary: The Deep Hot Biosphere by Thomas Gold (Abiogenic Oil)
FREE Book Summary: The Peanut Allergy Epidemic by Heather Fraser
FREE eBook: What is a woman? - “We don’t know yet.”
FREE eBook: A letter to my two adult kids - Vaccines and the free spike protein
Taubes G. Epidemiology faces its limits. Science. 1995;269(5221):164-169.
Massey Christine. Personal communication documenting replies to various Freedom of Information (FOI) requests from 58 governments of the world; these replies (as of July 25, 2021) indicate that 86 health/science institutions in 23 countries/jurisdictions have “no record” of “SARS-CoV-2” isolation/purification from any patient sample, “anywhere, ever.” Responding institutions include the Public Health Agency of Canada, the CDC, the UK Department of Health and Social Care and the Indian Council of Medical Re- search. See https://www.fluoridefreepeel.ca/fois-reveal-that-health- science-institutions-around-the-world-have-no-record-of-sars-cov- 2-isolation-purification/. This link corroborates the claims made by Dr. S. Alexov, who serves on the Board of the European Society of Pathology, a professional group representing pathologists in 30 European countries.
Engelbrecht T, Scoglio S, Demeter K. Phantom virus: In search of Sars-CoV-2. Off-Guardian, Jan. 31, 2021. https://off-guardian. org/2021/01/31/phantom-virus-in-search-of-sars-cov-2/.
Enders JF, Peebles TC. Propagation in tissue cultures of cytopathogenic agents from patients with measles. Proc Soc Exp Biol Med. 1954;86(2):277-286. doi: 10.3181/00379727-86-21073.
Enders JF, Peebles TC, McCarthy K, et al. Measles virus: a summary of experiments concerned with isolation, properties, and behavior. Am J Public Health Nations Health. 1957;(3):275-282. doi: 10.2105/ajph.47.3.275.
Giannessi F, Aiello A, Franchi F, et al. The role of extracellular vesicles as allies of HIV, HCV and SARS viruses. Viruses. 2020;12(5):571. doi: 10.3390/v12050571.
Caly L, Druce J, Roberts J, et al. Isolation and rapid sharing of the 2019 novel coronavirus (SARS-CoV-2) from the first patient diag- nosed with COVID-19 in Australia. Med J Aust. 2020;212(10):459- 462. doi: 10.5694/mja2.50569. Epub 2020 Apr 1.
Lanka S. Preliminary results: Response of primary human epithelial cells to stringent virus amplification protocols (unpublished). April 2021.
Davis I. COVID19 – Evidence of Global Fraud. Off-Guardian, Nov. 17, 2020. https://off-guardian.org/2020/11/17/covid19-evidence-of-global-fraud/.
Thank you all for the lively debate and exchanges.
Who would have thought that asking a few questions about genetic matter packed into a protein sandwich could create so much heat.
I know that most of you know this, especially those that read the whole article, but I don't have my mind made up on this issue. I am not a "no virus" guy. I might be that in the future, but that's not where I am right now.
I think the best description of my current state on this question is:
Covid and its vaccine was brought to me by the same charlatans that created virology.
On that basis, what are the chances that virology is wholly or substantially untrue and corrupt.
I think pretty damn high. Bordering on a certainty.
On that basis I would like to try to figure out what and where the untruths are.
Cowan makes some very specific points. If they can be refuted, then I welcome the refute.
This is important stuff. The whole globalist plan is built around the idea of public health.
The primary threat to global public health are viruses, we are told.
The primary solution to that threat are vaccines (a virology product).
So, said another way, the whole world is now being run on ideas birthed out of virology.
If there is any subject at all, that merited rigorous interrogation, seeking its truth; this is it.
First, I really appreciate this substack!
Cowan, the Baileys, Kauffman (and others) have been championing this "no-virus" information for years now. My journey to realization happened much like yours, but I am a bit further down the road than you are.
My virus awakening:
Whut???? Surely the experts know what they are talking about.
That's weird.
Never isolated? Prove it.
Proved, but we must still misunderstand what they mean.
No, I understand and somebody is BAD WRONG. But which 'side'.
These bastards have lied to us.
Hang 'em high!
\
That's about where I reside right now. The next step for me is offering to pull the levers that hang them when they are prosecuted.
Now, the covid stellar bettor Steve Kirsch had his admin ban me (twice). First time was temporary because I kept asking Steve (on his substack and emails) to sit down on video (or in person, even better) with his choice of debate mates (I suggested Malone, McCullough, or Kory) opposed to Bailey, Cowan and Kauffman (or whatever team they decide to assemble) to hash out the glaringly obvious real questions these anti-virus people are articulating (good enough to educate this dumb ole redneck).
They grew tired of my insistence and banned me for a month. No, I was not being ugly. Just insistent.
The second time Kirsch's admin banned me (a month or 2 later, and permanent) was when I asked Steve (on substack and emails) why he would not bet Ron Unz after Unz took him to task over death numbers on the phone (multiple calls/discussions) where Unz claims Kirsch agreed with him, yet every post at his substack was ignoring Unz's claims.
I pointed them out and asked why the king of bettors was not betting Unz.
BANNED.
I am to the point that I see this entire thing as a scam (virology) and we have several gate keepers that are ostensibly COVID hunters, yet they refuse to acknowledge (or even debate) what many see as obvious.
There. I said it.
So, if viruses are not real, then we have what is an obvious genocide with the covid attack.