


Whooping Cough (Pertussis)
On Bacteria


We know that all virus stories lead to vaccines.
This is a bacterial story that leads to vaccines.
It’s taken me a while to understand the essence of the argument that Cowan et al have made about viruses. But I now accept it.
I would frame the essence of the argument as such: Virology has not been able to prove that the particles they call viruses cause disease.
Which is why I don’t like calling them Team No Virus. It would be truer to call them Team No Proof. All they, and now I, are saying is “Prove it.” If they can, I would be happy to go back to believing in viruses as causal agents.
If you are new to this subject, as I once was, I would recommend reading these stacks that are an outline of the journey I’ve been on:
When it comes to bacteria, I am still trying to figure it out.
I accept the general argument that Cowan et al have put forward, which is that bacteria arrive at the sight of an infection as part of the bodies natural healing process, to “eat” the infection and dead tissue. That they are already in the body and are called upon when needed.
They are the fire fighters that are blamed for the fire.
I believe this explanation is both intuitive, elegant and functionally true. But…
I need to better understand why antibiotics “work,” and what does “work” mean in the context of firefighters?
I’m glad to see I’m not alone in my confusion.
Here are two interesting comments to a recent Rancourt stack.
Germ theory critical excess? - by Denis Rancourt
This from Mike Yeadon:
One point about antibiotics. I can’t speak for all of the not very many structural types, but some of them are intrinsically anti-inflammatory, independent of their ability to prevent bacterial replication in Petri dishes. It occurred to me when I was in Pfizer that their leading antibiotic might work in its leading indication, acute exacerbations of chronic obstructive pulmonary disease, by being anti inflammatory.
In practise, more or less impossible for distinguish.
I mention it, because I detected that you were convinced that, because agents termed antibiotics were useful in lung disease, this was pretty much proof of a pathogenic role for bacteria.
I’m only very slightly waggling that stake, because I pretty much agree with you (my remarks notwithstanding).
I think sequencing is going to turn out to be total fraud and nonsense. I already know enough to disregard the argument that “so many independent scientists found the same sequences, so there must be a contagious virus”.
First, I challenge the diversity of the sources. If they use the same machine’s & algorithms, that’s not diversity. And I think they do, or at least the methods & results are not truly independent. They also draw upon common databases and assumptions.
Next, the method used to determine (or is it form?) the “full length sequence” is not scientific. There’s extensive generation of short sequences, assumed to be contiguous, which are then assembled in the most plausible order using clever software. I understand the software makes no progress whatsoever until it’s presented with a potential skeleton, whereupon it assembles the contigs in a way that mimics it, with small variations. I don’t know enough to really understand the shell game that I suspect must be going on here. I have faith that you can get to the bottom of it, if you’ve time and inclination.
This was my favourite comment from Gordon:
I love and respect these guys, as well. The first wave of thinkers always has to wave the flag just a bit too hard, and that's what I think is going on here.
A good example is what Dr Cowan says about sepsis: It's not the bacteria in your blood that is damaging, but the waste products they generate. To be honest, that's probably true but when you say "it's not the bacteria that are harming you, it's their poop", the distinction can put the clinical outcome at risk... If you have sepsis, get IV antibiotics and kill the things that are pooping in your blood. Rebuild your microbiome when you're not at risk of imminent death.
I'm very much a terrain guy but I reserve the right to nuke bugs, lol.
Unrelated to my comment, this is the tightest take-down of PCR's shortcomings I've ever read, Denis:
"I remain highly suspicious of a wet chemical method (PCR) that relies on controlled thermal degradation to amplify a molecular fragment a kazillion times, which could not otherwise be detected. And I remain skeptical that thus obtained genome sequences are particularly relevant to biology. That’s me."
There is heated debate and arguments in the comments section that I have summarized along these lines:
Why viruses do not cause disease:
Every study attempting to demonstrate viral transmission through natural means (like breathing aerosolized "virus") has failed to produce disease
There is no direct evidence of viruses being isolated from human tissue or fluids using electron microscopy without cell culture manipulation
PCR testing is fundamentally flawed as it relies on thermal degradation and amplification of fragments that may not represent actual viruses
Historical disease outbreaks attributed to viruses often have plausible alternative explanations (environmental toxins, malnutrition, etc.)
The common symptoms attributed to viral infections can all be explained by the body's natural detoxification processes
Why viruses do cause disease:
The genomic sequencing of viruses shows consistent patterns of evolution and variation that match disease spread
Antibody studies demonstrate specific immune responses to viral proteins that emerge with new diseases
The rapid spread of diseases through previously isolated populations (like Hawaii natives) suggests transmissible pathogens
Recurring patterns of disease transmission within households and communities follow expected viral behavior
Government investment in viral bioweapons research suggests viruses have real effects
Why bacteria don't cause disease:
Bacteria are primarily scavengers that consume dead/dying tissue rather than causing the initial damage
Many "pathogenic" bacteria are found naturally in healthy people without causing disease
The presence of bacteria does not prove they caused the disease - they may arrive after tissue damage
Koch's postulates for proving bacterial causation of disease have never been fully satisfied
Disease outcomes depend more on the host's terrain/health than presence of bacteria
Why bacteria do cause disease:
Antibiotic resistance develops through bacterial evolution, showing bacteria actively adapt to survive
Specific bacterial infections produce consistent, predictable symptoms across patients
Bacteria produce toxins that can damage healthy tissue beyond just cleaning dead material
The progression of symptoms in conditions like pneumonia follows bacterial growth patterns
Bacterial infections can be transmitted between hosts with similar genetic profiles
Why antibiotics work:
They have anti-inflammatory properties independent of their antimicrobial effects
They can help regulate the microbiome when it becomes imbalanced
They may neutralize bacterial toxins that cause inflammation
They reduce bacterial populations that could overwhelm the body's healing capacity
They provide time for the immune system to mount an effective response while reducing bacterial load
I’ve digressed, let’s get back to whooping cough (pertussis).
What is clear from the excerpt below is that what should have been a straightforward bacterial story, is anything but.
So, despite the declaration that Bordetella pertussis was named as the cause of whooping cough in 1906, more than a century later, there does not appear to be a single scientific publication that establishes that this is in fact the case. It remains entirely probable that when an individual becomes unwell, they are more likely to have an overgrowth of bacteria such as Bordetella pertussis due to the changing terrain, including dying cells, in the respiratory tract. And despite the claims that “people with pertussis usually spread the disease by coughing or sneezing,” it has never been demonstrated that spraying the bacteria into the air can make any nearby humans or animals sick. Studies of the nasal microbiome in healthy volunteers have shown that there are always billions of bacteria present, and some are even termed “pathogens.” Obviously, the mere presence of these microorganisms is insufficient to cause disease alone.
And this on the absence of control groups (the same trick used with viruses).
However, there was no control group of animals to see whether simply pouring other types of brews directly into their lungs would result in similar effects. In other words, none of these experiments followed the scientific method and there was no determination that a bacterium was the cause of the symptoms.
So what causes whooping cough?
On that account, what is the conceivable cause of whooping cough if it has never been proved that this bacterium alone can cause the disease? Due to the persistent research and confirmation bias that centers on the Bordetella model, that question remains unanswered.
So here we are again, with something that should have been easily proved and answered by now, but instead we find the same malfeasance, obfuscation and scientific fraud.
Why?
For me, there is only one answer, and that is because “Bordetella pertussis doesn’t cause whooping cough.” If it did, ample honest evidence would be readily available.
I’m not prepared to generalize just yet to all bacteria, but just on this issue, it seems we are in the midst of an all too familiar rotten and putrid captured industrial science, or The Science.
I think whooping cough is particularly valuable to Cartel Medicine as it opens the door for more vaccines against “bacterial disease” not just “viral disease.”
One of the areas they have used this to “expand their market” is by scaring new parents and their extended family into getting a pertussis vaccine to be able to see the new baby, otherwise they need to stay away for several weeks.
This is the official line:
Here are the key points regarding extended family getting the pertussis (whooping cough) vaccine to visit a newborn:
1. It is generally recommended that close household contacts and caregivers of infants under 6 months old get the pertussis vaccine (Tdap) if they haven't had it in the last 10 years[1][3][7].
2. The most important way to protect a newborn is for the mother to get vaccinated during pregnancy, ideally between 28-32 weeks. This passes antibodies to the baby before birth[8][9].
3. Other household members like the father, siblings, and grandparents should also be up-to-date on their pertussis vaccination[8].
4. For extended family or occasional visitors, getting vaccinated can provide some additional protection[8][9].
5. Some parents choose to implement a "No Vax, No Visit" policy for all visitors[10].
6. Visitors should postpone their visit if they are sick and practice good hand hygiene before contact with the baby[10].
7. The CDC recommends that anyone who will be in close contact with the baby get vaccinated at least 2 weeks before meeting the infant[6].
8. Some healthcare providers recommend all visitors be vaccinated, while others focus on household members and regular caregivers[2][5].
Footnotes1
With thanks to the Drs Bailey for their masterpiece The Final Pandemic.
The Final Pandemic: An Antidote To Medical Tyranny: Bailey, Dr Samantha, Bailey, Dr Mark,
The PCR Exposed Whooping Cough’s Faulty Science
Excerpt from The Final Pandemic
In its “Whooping cough” entry, online encyclopedia Wikipedia plainly states, “pertussis is caused by the bacterium Bordetella pertussis” and provides a single reference for the claim. The reference is a CDC webpage, and like many public health authorities, it emphatically states that, “pertussis, a respiratory illness commonly known as whooping cough, is a very contagious disease caused by a type of bacteria called Bordetella pertussis.”
The CDC webpage cited two references for its claim. The first reference was a 2004 epidemiological paper that simply interviewed family members to identify the “source” of the alleged infection in 264 out of 616 (43%) infant cases. The second CDC reference, “Transmission of Bordetella pertussis to Young Infants” was a prospective study investigating 404 “contacts” of 95 infant pertussis cases. The methodology in this paper involved diagnostic evaluation (including PCR and a blood test) being performed on all participants independent of symptoms. It concluded that the “source” had been identified in 48% of cases. In other words, despite their trawling efforts they were unable to identify the alleged source in over half the cases, and if they did find the “source,” the supposed culprit could be completely well. More crucially, neither study possessed suitable methods to determine if the bacteria caused disease or whether humans could transmit the condition of pertussis.
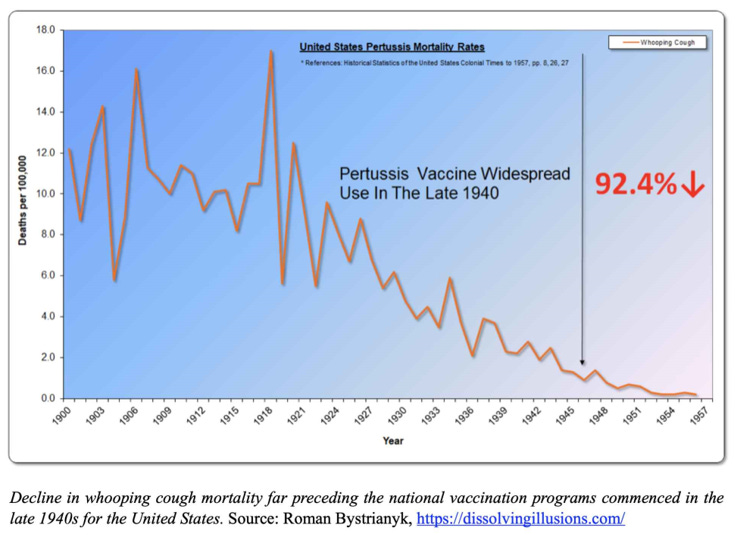
It is also noteworthy that this second paper makes the claim that, “pertussis vaccination has reduced the number of notified cases in industrialized countries from peak years by more than 95%.” This is deceptive because vaccines could not have been a significant factor for the dramatic decrease in disease burden that has been witnessed. As documented in the book Dissolving Illusions, by the time widespread pertussis vaccination was introduced in the 1950s, whooping cough had become a mild disease, and mortality had plummeted by over 90% in the US and 99% in the UK.
Additionally, in a 1995 letter from Victoria Romanus at the Swedish Institute of Infectious Disease Control, there was the indication that nationwide deaths from whooping cough were only 0.6 children per year from 1981 to 1993 in Sweden when there was no national vaccine program. Clearly the pertussis vaccines were not responsible for the massive reduction in deaths which is what most of the public have been led to believe. (The authors recommend that the reader consults Dissolving Illusions where similar conclusions are demonstrated for the relationship of vaccines to all the best known childhood diseases.)
From these two studies the CDC cited it is simply not possible to conclude that; (a) Bordetella pertussis is the causal agent for whooping cough or that, (b) human to human transmission of disease occurs. At most, it can be concluded that the presence of the bacteria possesses an association with the clinical picture of whooping cough and that sometimes there are clusters of illness in people sharing common environmental conditions.
It is already apparent that the use of the PCR to detect “cases” is highly dubious. Even if the PCR has very specific primers and is done with the utmost care, what is the clinical significance of finding some genetic sequences from the bacteria? The bacteria may be already dead, or if alive, simply present in such small numbers that they will cause no problem for the lungs. Crucially, the PCR itself cannot determine whether an individual is well or unwell in these circumstances.
If we examine the history of the apparent identification of the bacteria responsible for whooping cough, we can see that the idea of a “contagious pathogen” was imagined very early on. In 1765, Swedish doctor Nils Rosen von Rosenstein, considered one of the pioneers in the field of paediatrics, commented that:
The true cause of this disease must be some heterogeneous matter or seed which has a multiplicative power as is the case with smallpox…we find that it is communicated by infection and that a part of it is attracted by the breath down into the lungs.
Then in 1901, when the focus on germ theory had become much stronger, Marcus Hatfield, Professor of Diseases of Children at the Chicago Clinical School, wrote:
Contagiousness is great, a chance meeting, a few moments conversation, or a seat next to the sick child is generally sufficient to convey the disease, which may also be carried upon linen, or clothing soiled with the expectoration of one suffering from whooping cough…It is generally conceded that a microorganism is the exciting cause of pertussis, but its natural history has not yet been definitely settled, although since 1867 bacteriologists have at short intervals been discovering the alleged peccant microbe.
Belgian microbiologists Jules Bordet and Octave Gengou took up the challenge to confirm the alleged offending microorganism, and in 1906 it was declared that they had found it, as described in this 2010 account by Patrick Guilfoile:
Bordet and Gengou initially took respiratory secretions from a five-month-old infant who had whooping cough and placed the material on their growth medium. Many small bacteria, now identified as Bordetella pertussis, grew on the plate. Subsequently, they placed plates containing this medium under the mouths of children who had whooping cough, during a coughing spell, and isolated the same pathogen from these other patients.
Hence, from 1906 onwards, Bordetella pertussis has generally been considered the causal agent of the clinical condition known as whooping cough. However, what was described by Bordet and Gengou did not establish that this bacterium was inhaled by people to cause illness. Instead, they simply found it in the respiratory secretions of some individuals who had a persistent cough. The relentless coughing is merely an indication that an abnormal state exists in the respiratory tract. Their only significant finding was an association with the presence of, or at least increased amounts of Bordetella pertussis.
In the modern era, animal studies have been cited as apparent evidence that Bordetella pertussis causes whooping cough. However, these studies can hardly be said to establish any such claims when one examines the methodology. For example, the researchers were “infecting” rhesus macaques by introducing concentrated bacterial cultures directly into their nostrils and lungs via endotracheal tubes while under ketamine anesthesia. Following this procedure, which cannot be said to replicate anything that would happen in nature, they concluded that:
All four monkeys were infected, as demonstrated by our ability to isolate B. pertussis from nasopharyngeal washes from day 3 until approximately day 15 postinoculation. Two of the four monkeys developed a significant rise in white blood cells (4- and 6-fold). One of the two monkeys with an elevated white blood cell count developed a mild cough that persisted for several days.
In summary, half of the monkeys had a rise in their white blood cell count, which would be an expected inflammatory response when foreign material is poured directly into their lungs, and only one developed a cough, which again would be expected by the artificially-induced lung irritation. They then claim they had “demonstrated” infection by finding the bacteria in the same place they had poured them into, for the following two weeks. Even more “success” was achieved by making baby baboons cough by injecting the concentrated bacterial brew directly into their lungs. However, there was no control group of animals to see whether simply pouring other types of brews directly into their lungs would result in similar effects. In other words, none of these experiments followed the scientific method and there was no determination that a bacterium was the cause of the symptoms.
Yet other experiments that claim to demonstrate “infection” with pertussis among baboons also labour under dubious interpretations. In a 2014 US Food and Drug Administration study, young baboons were “infected” with Bordetella pertussis by again pouring concentrated bacterial cultures directly into their lungs. They found that co-housing these “infected” baboons with other baboons caused the latter to become “colonized” with Bordetella pertussis. But these “colonized” baboons did not develop whooping cough or become unwell. Instead, the researchers simply detected the bacteria in their respiratory tracts. Further, the degree of colonization was indistinguishable between the animals that had been vaccinated and those unvaccinated, an inconvenient result for the claim that the vaccines offer protection.
So, despite the declaration that Bordetella pertussis was named as the cause of whooping cough in 1906, more than a century later, there does not appear to be a single scientific publication that establishes that this is in fact the case. It remains entirely probable that when an individual becomes unwell, they are more likely to have an overgrowth of bacteria such as Bordetella pertussis due to the changing terrain, including dying cells, in the respiratory tract. And despite the claims that “people with pertussis usually spread the disease by coughing or sneezing,” it has never been demonstrated that spraying the bacteria into the air can make any nearby humans or animals sick. Studies of the nasal microbiome in healthy volunteers have shown that there are always billions of bacteria present, and some are even termed “pathogens.” Obviously, the mere presence of these microorganisms is insufficient to cause disease alone.
Unfortunately, germ theory tunnel vision means that mainstream researchers continue to create new narratives to explain the glaring inconsistencies and the manifestly unscientific vagaries of their research. For example, in 2020, a pertussis systematic review paper found that many “cases” had minimal or no symptoms and concluded that, “the studies included in this review report a high incidence of asymptomatic and mild/atypical infection among household contacts of pertussis cases.” This echoed another paper from 2015 that stated, “asymptomatic transmission is the most parsimonious explanation for many of the observations surrounding the resurgence of B. pertussis in the US and UK.” Surely implying that entirely healthy people are now “infected” or have become carriers of disease is starting to stretch the theory very thin?
For many researchers, however, adherence to germ theory continues to cement the tendency that all roads to lead to vaccines. For example, a 2013 paper on “Pertussis resurgence” advises us, “to select vaccines and vaccination strategies that are most effective” and goes on to claim, “pathogen adaptations reveal weak spots in the bacterial defense and hence point to ways to improve vaccination.” Trying to explain the mild persistence of whooping cough through “pathogen adaptation” and waning vaccination immunity is simply another case of the germ theorists trying to fit observations of the natural world into their model. The consequence of this impaired theory is that it fails to identify and correct the real causes of illness.

On that account, what is the conceivable cause of whooping cough if it has never been proved that this bacterium alone can cause the disease? Due to the persistent research and confirmation bias that centers on the Bordetella model, that question remains unanswered. However, we can reasonably suspect that various environmental and nutritional factors contribute to the individual’s ‘terrain’ and thus susceptibility to illness.* Unfortunately, studies tend to focus on factors such as household contacts rather than the underlying physical characteristics of the cases. For example, a 2017 epidemiological study concluded that:
Sharing a household with a young adolescent was a significant risk factor for pertussis in adults and older teenagers. The primary focus of the childhood pertussis vaccination programmes is to prevent infant disease. Although evidence is emerging that adolescent vaccination does not provide indirect protection to infants, our results highlight the importance of children aged 10–14 years in pertussis transmission to older adolescents and adults.
While the observation that, “sharing a household with a young adolescent” was identified as a risk factor, it is simply an association and cannot be claimed to demonstrate causation. In this case, the implication is that the adolescent is infecting others in the house with B. pertussis. While epidemiological studies may provide some clues as to what may be contributing to disease, they can be dangerously misleading if conclusions rely on unproven assumptions. It is highly relevant that the CDC has reported around 90% of whooping cough cases occur in the developing world. While the CDC claims this is due to low vaccination rates, it ignores the stark reality that children in the developing world have much higher rates of nutritional deficiencies and exposure to a host of potentially compromising environmental factors.
It is also known that with regard to fatal cases of whooping cough, the children have significantly lower birth weight and younger gestational age compared to non-fatal cases. It is a tragedy that more data has not been gathered surrounding underlying physical, nutritional, and toxicological factors. This appears particularly so with regard to “conventional” treatments such as antibiotics. Even a Cochrane Collaboration Review concluded that:
The findings of this review suggest that administration of antibiotics for the treatment of whooping cough is effective in eliminating B. pertussis from patients with the disease to render them non-infectious but does not alter the subsequent clinical course of the illness...There is insufficient evidence to determine the benefit of prophylactic treatment of pertussis contacts. Prophylaxis with antibiotic was significantly associated with side effects and did not significantly improve clinical symptoms, whoop, paroxysmal cough, number of cases who develop culture positive B. pertussis or paroxysmal cough for more than two weeks in contacts older than six months of age.
The only criticism we would add to this otherwise accurate conclusion is that eliminating B. pertussis in patients would, “render them non-infectious,” which is a blatant example of illogical circular thinking. As the scientific evidence shows, no patient has ever been shown to be “infectious” regardless of whether the bacteria can be found in the person or not. In other words, there is no evidence that people “pass on” or “catch” whooping cough.
*In reading this book, Dr M.C.J. McGrath eloquently remarked that, “the monstrously magnified result has the effect of turning a whispered hint into a bullish roar, inverting uncertainty into imagined certainty while simultaneously conveying an illusion of authoritative ‘science' and providing justification for an infinite constellation of controlling social interventions. The manufacturing of ‘cases’ is the very backbone of the gaslighting illusion of a ‘pandemic’, whose definition by the WHO is now meaningless, constituting no more than a readily ‘transmittable’ idea.”
I appreciate you being here.
If you've found the content interesting, useful and maybe even helpful, please consider supporting it through a small paid subscription. While everything here is free, your paid subscription is important as it helps in covering some of the operational costs and supports the continuation of this independent research and journalism work. It also helps keep it free for those that cannot afford to pay.
Please make full use of the Free Libraries.
Unbekoming Interview Library: Great interviews across a spectrum of important topics.
Unbekoming Book Summary Library: Concise summaries of important books.
Stories
I'm always in search of good stories, people with valuable expertise and helpful books. Please don't hesitate to get in touch at unbekoming@outlook.com
For COVID vaccine injury
Consider the FLCCC Post-Vaccine Treatment as a resource.
Baseline Human Health
Watch and share this profound 21-minute video to understand and appreciate what health looks like without vaccination.
[1] https://immunisationhandbook.health.gov.au/recommendations/adult-household-contacts-and-carers-of-infants-aged
[2] https://www.hopkinsmedicine.org/health/wellness-and-prevention/new-parents-and-newborns-are-visitors-ok
[3] https://www.cdc.gov/vaccines-pregnancy/about/vaccines-family-caregivers.html
[4] https://www.findapharmacy.com.au/__data/assets/pdf_file/0027/65376/Visiting-a-new-baby-a-guide-from-your-community-pharmacist.pdf
[5] https://www.reddit.com/r/pregnant/comments/1444plk/whooping_cough_vaccine_did_you_make_all_visitors/
[6] https://www.marchofdimes.org/find-support/blog/two-vaccines-every-grandparent-needs
[7] https://www.thetraveldoctor.com.au/whooping-cough-vaccination-babys-caregivers/
[8] https://www.abc.net.au/news/2019-06-26/setting-the-rules-for-visitors-after-you-have-a-baby/11229516
[9] https://www.cdc.gov/pertussis/vaccines/recommendations.html
[10] https://www.sydney.edu.au/news-opinion/news/2016/06/01/_no-vax--no-visit-.html
[11] https://www.amcal.com.au/our-pharmacists-services/familyvaccinations/
[12] https://pmc.ncbi.nlm.nih.gov/articles/PMC3922557/
[13] https://www.rch.org.au/kidsinfo/fact_sheets/whooping_cough/
[14] https://www.health.nsw.gov.au/immunisation/Documents/wc-newborns-factsheet.PDF
Back in the 80's the WHO admitted that the single most effective way to prevent and treat measles (in an African study) was to give the kids vitamin A. So clearly what we're seeing is a symptom of malnutrition. So did anyone at the WHO decide to distribute the cheap solution to Africans?
NOPE. Instead they went around injecting (maiming and even killing) African kids.
Great article! I don't know if there are "good" and "bad" bacteria. Maybe some bacteria are "bad,' but, like parasites, if they kill the host, where will they live? We can't live without bacteria!
Dr. Tom Cowan is a co-founder of the Weston A Price Foundation. Dr. Price did thousands of experiments by taking infected teeth from sick people and putting them into rabbits. The rabbits got the disease the human had. So, what transferred the disease? What is an infection? I've come to believe that an infection is injured and decaying tissue, not bacteria. I think our bodies send all the healing forces to an area of injury, which creates the infection symptoms. It's not the bacteria. It's the decay and maybe something there that the body can't dispose of such as a chipped bone or some foreign object.
I think with bacteria, it's not "good" or "bad." It's all about balance and habitat. If we do something that kills off a particular bacterial species, an imbalance is created. "Covid" and the jabs kill off the bifidobacteria. Who is going to do their jobs? ... Also bacteria sometimes migrate to the wrong habitat. Think SIBO. Small Intestinal Bacterial Overgrowth. So bacteria may belong in the colon, but they migrate to the small intestine. They don't belong there. The bacterial colonies are out of balance.
Something in our environment is harming the bacteria that make B vitamins. Likely it is glyphosate and High Fructose corn syrup (which is a pesticide) as well as other things. Bacteria make neurotransmitters. They seem to be short of employees. We seem to have mixed up neurotransmitters.
When it comes to terrain, something that is overlooked is the EMF environment. This is a huge topic particularly with all the Gs... 2G, 3G 4G, 5G, dirty electricity, fluorescent lights, wi-fi, etc. The EMF environment determines who can thrive, who cannot, what grows, as well as behavior. The current EMF environment encourages abnormal growth and aberrant behavior in plants, animals, and humans.