
The Stent You Don't Need
An Essay on the Coronary Artery Myth and What Actually Causes Heart Attacks

Every cardiologist’s office has the same picture. Three large arteries — the right coronary, the left anterior descending, and the left circumflex — rendered in orange or red, branching neatly across the surface of the heart like rivers feeding a valley. The image is so familiar that most patients never ask an obvious question: is this what a heart actually looks like?
It isn’t. The standard coronary artery diagram is an artist’s rendering or a computer-generated image. It is not a photograph, not a scan, not an observation. It is a construction — and the entire edifice of modern interventional cardiology rests on it.
The Picture They Don’t Show You
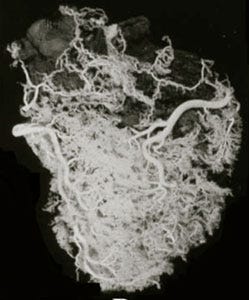
The Italian pathologist Giorgio Baroldi spent decades studying the actual vasculature of the human heart. Using injection and corrosion casting techniques, he and his colleague Malcolm Silver developed methods to visualize the full blood vessel network of a healthy heart — not just the three major coronary arteries, but every vessel that carries blood to the cardiac tissue.¹
The resulting images look nothing like the cardiologist’s diagram. Where the standard picture shows three rivers, Baroldi’s work reveals something closer to a watershed — a dense, saturated network of small vessels covering the entire surface of the heart, front and back. The three major coronary arteries are still visible within this network, but they are embedded in it, not the sum of it. An estimated 90 to 95 percent of blood flow reaches the heart muscle through small vessels that do not appear on a coronary angiogram.²
This is not a disputed finding. It is an anatomical fact that anyone with the right technique can verify. The question is why cardiology has shown so little interest in verifying it.

The Fundamental Mistake – Heart Attack: Alternatives to Conventional Medicine
Support Independent Investigative Journalism and Research
This work remains free because paid subscribers make it possible. If you find value here, consider joining them.
What paid subscribers get: Access to all books I’ve written plus 1-2 new ones per month. e.g.
The DMSO Book
The Kitchen Remedies Guide
Chlorine Dioxide
The PSA Trap
Breast Cancer
Drilling for Profit
What Your Vet Can’t Tell You
Plus: Access to the Deep Dive Audio Library — 180+ in-depth discussions (30-50 min each) exploring the books behind these essays. New discussions regularly added. That’s 100+ hours of content for less than the price of a single audiobook.
[Upgrade to Paid – $5/month or $50/year]
How Angiograms Create a False Reality
A coronary angiogram works by threading a catheter into the coronary arteries and injecting heavy metal dye under high pressure while taking X-ray images. The test visualizes the three major coronary arteries because those are the vessels large enough for the catheter and dye to reach. The vast collateral network — the watershed — is invisible to this method.
The result is a diagnostic artifact. The angiogram creates the impression that all blood flows through three vessels because it can only see three vessels. A patient shown their angiogram results sees what appears to be a complete picture of their heart’s blood supply, with a frightening narrowing in one artery. The cardiologist points to the blockage. The patient agrees to the stent.
The artifact goes further. Injecting heavy metal dye under high pressure into an artery causes the muscular wall of the vessel to spasm. If a plaque is blocking 50 percent of the artery’s interior, the spasm narrows the vessel around it, and suddenly the blockage appears to be 70 percent or more.³ This overestimation of stenosis is built into the test itself. It is not a rare error. It is what the test does, every time, to varying degrees.
Dr. Knut Sroka, a German cardiologist and researcher, produced detailed video demonstrations of this phenomenon through his work documenting the collateral circulation that angiograms fail to capture.⁴ His central point is straightforward: coronary angiograms are notoriously inaccurate tools for assessing stenosis and blood flow in the heart, and most of the procedures they justify are performed on patients whose blockages are already fully compensated by collateral vessels.
This is Sroka’s heart catheter film — the one referenced in this essay. Here’s the translation and summary:
Translation
“In this short film, the right coronary artery — here on the left side of the image — is filled with contrast dye via a heart catheter.
The decisive finding of this examination, stated upfront for your orientation: there is a high-grade narrowing in the middle section of the artery — a stenosis, as it is called. Now to the coronary film.
[Film plays, then replays]
Now I will show you a series of still images taken from the coronary film so you can study the processes in detail at your leisure.
Here is the first image. At the top of the frame you can see the heart catheter lying with its curved tip, still without contrast dye.
The first contrast dye. The artery is marked in its uppermost section.
This photo is the most exciting of all. Why? you will rightly ask.
It concerns primarily the marked dark stripe at the lower left. That is contrast dye in a section far beyond the stenosis. We see nothing yet of the narrowing itself, and yet a distant section of the coronary artery is already filling.
Here, for the first time, the stenosis begins to appear — circled.
The same image again. The bottleneck is beginning to become visible through descending flow from above and, crucially, through ascending flow from below.
It becomes clearer: this stenosis allows hardly a drop of blood to pass through.
Practically nothing gets through the bottleneck. It is therefore not the case — as a layperson might imagine — that blood forces itself through the needle’s eye and fills the lower section of the artery poorly. Yet precisely this section beyond the narrowing is well filled. The blood must be coming from somewhere.
Even though the collaterals — the vessels that bypass the bottleneck laterally — cannot be seen precisely, these images prove their existence and their effectiveness.
And here now, the perfect depiction of an approximately 90 percent stenosis. At the same time, this method misses something decisive. With the heart catheter, it is not possible to visualize the extensive network of fine collateral vessels. This results in considerable misjudgments regarding the significance of the coronary artery narrowing.
Into the extremely narrow bottleneck, a little blood squeezes from above, a little blood from below. Within the stenosis, the blood stands still.
If the narrowing is eventually sealed completely by a blood clot — a thrombosis — well, what then? Does a heart attack occur, as is generally assumed? Not at all. The blood is already standing still in the stenosis. A complete closure of the bottleneck would have no consequences whatsoever. Nothing would change.
It could not be more vivid. The blood supply to the heart muscle in the territory of the narrowed artery is absolutely undisturbed.
The right coronary artery is powerfully and clearly visualized down to its finest branches. The heart muscle suffers no damage from the high-grade bottleneck.
To further familiarize yourself with the invisible collaterals, it is best to watch the whole thing again right away.”
Summary
This is Dr. Knut Sroka’s narrated catheter film demonstrating the core argument against the coronary artery stenosis model. A patient has an approximately 90 percent blockage in the right coronary artery. During the angiogram, contrast dye reveals that the section of artery beyond the blockage fills with blood before the dye has even reached the stenosis — meaning blood is arriving from somewhere other than the blocked artery. The collateral vessels are doing the work, but the catheter method cannot visualize them.
Sroka’s key point: practically no blood passes through the stenosis, yet the heart muscle downstream is perfectly supplied. A complete thrombotic closure of the bottleneck would change nothing because the blood is already standing still within it. The heart catheter method systematically misrepresents the significance of coronary blockages because it cannot see the collateral network that has already compensated for them.
This is the film Cowan references in Human Heart, Cosmic Heart and the visual proof behind the watershed argument in the essay — the collateral circulation is not a backup system. It is the primary blood supply, and the angiogram is structurally incapable of showing it.
The Body’s Own Bypass
Starting soon after birth, the normal human heart develops an extensive network of small blood vessels called collateral vessels. These collateral vessels compensate for interruptions in flow through any of the major coronary arteries.⁵ This is not a pathological response to disease. It is normal cardiac development.
Large, stable blockages — those that obstruct more than 90 percent of a major coronary artery — are in almost all cases completely compensated for by this collateral circulation.⁶ The body has already performed its own bypass surgery, silently and without complication, using the very small vessels that do not appear on an angiogram.
This raises a question that the standard model cannot comfortably answer: if a person has a 90 percent blockage in a coronary artery and is walking around alive, how is their heart getting blood? If the three-river model were correct, that person should already be dead. The fact that they are alive, often with minimal symptoms, is itself evidence that blood is reaching the heart through pathways the angiogram cannot see.
Does it make sense that a person would have a heart attack when the stenosis goes from 93 percent to 98 percent? That is the implicit claim behind most stenting and bypass procedures — that clearing a blockage which the body has already routed around will prevent a future cardiac event. Study after study shows this is not the case.
What the Trials Actually Show
In 2003, the Mayo Clinic published a major report evaluating the efficacy of bypass surgery, stents, and angioplasty for chronic stable angina. The findings were stark:⁷
Bypass surgery relieves symptoms — specifically, chest pain. Bypass surgery does not prevent future heart attacks. Only patients in acute, life-threatening danger show improved survival from bypass surgery.
The gold standard treatment for coronary artery blockages, in other words, does not accomplish the thing patients believe it accomplishes. It reduces pain but does not prevent the event that patients most fear. The surgery works as a palliative, not a preventive.
At a cardiology conference in Northern California, a cardiologist reported on a trial conducted during his residency in rural Alabama. Researchers performed angiograms on men presenting with chest pain. Those found to have a single blocked artery received no treatment. The researchers recorded their predictions about where a future heart attack would occur — naturally, they predicted the area of the heart supplied by the blocked artery. Many of the men did eventually have heart attacks. Fewer than 10 percent had the heart attack in the predicted location.⁸
The blocked artery did not determine where the heart attack happened. The plumbing model failed at its most basic predictive task.
The Pathology Evidence
Autopsy studies provide the most reliable evidence of what actually happens during a heart attack, because they examine the physical tissue rather than relying on the artifacts of angiography.
The first major pathology study of heart attack deaths, conducted in the 1970s, found that stenosis sufficient to have caused the heart attack was present in only 20 percent of cases.⁹ In the largest such study ever conducted — published in 2004 by Baroldi and Silver themselves — sufficient stenosis was found in 41 percent of cases.¹⁰
Flip those numbers: in 59 percent of heart attack deaths in the largest autopsy study ever done, the blockage was not severe enough to have caused the event. In the earlier study, the figure was 80 percent. Whatever killed these people, it was not a blocked coronary artery.
Baroldi and Silver also documented a methodological problem that inflates the apparent correlation between stenosis and heart attacks. They found that the larger the area of tissue death, the more often stenosis was present — and the longer the interval between heart attack and death, the higher the percentage of stenosis. Researchers who focus only on major heart attacks or patients who survived long enough to reach the hospital will find stenosis rates that appear to support the coronary artery model. The full dataset does not.
Thrombosis — blood clots in the coronary vessels — is a real phenomenon associated with heart attacks. But in no pathological study has thrombosis been found in more than 50 percent of heart attack deaths.¹¹ In many cases, the thrombosis develops after the heart attack has already begun, making it a consequence rather than a cause.
The Oxygen Paradox
The coronary artery theory proposes a clear mechanism: blocked artery leads to reduced blood flow, which leads to oxygen deprivation, which kills heart cells. If this mechanism were correct, you would expect to find falling oxygen levels in the heart tissue during an evolving heart attack.
Careful measurements of myocardial oxygen levels (pO₂) during heart attacks show no oxygen deficit.¹² The oxygen levels in the heart cells do not change throughout the entire event. The tissue dies, but not from lack of oxygen.
This is not a minor discrepancy. It is the complete absence of the mechanism that the entire coronary artery theory depends on. If the oxygen supply to the heart doesn’t change during a heart attack, then whatever is killing the myocardial cells, it is not arterial blockage cutting off their oxygen.
What the Risk Factors Actually Tell Us
Any credible theory of heart attacks must account for the known risk factors: being male, having diabetes, smoking, and chronic psychological or emotional stress. None of these risk factors directly affect the coronary arteries. Diabetes and smoking cause disease in the capillaries — the small vessels — not the large ones. Stress has no known direct effect on coronary arteries. The risk factors for heart attacks point away from the large vessels and toward something else entirely.¹³
The same disconnect appears in cardiology’s own medications. The four main drugs used to treat heart disease are beta-blockers, nitrates, aspirin, and statins. Each provides some benefit to heart patients. None works primarily by addressing plaque or stenosis.
Beta-blockers block the sympathetic nervous system — the fight-or-flight response. Nitrates stimulate nitric oxide production, which activates the parasympathetic nervous system. Aspirin and statins also stimulate nitric oxide and acetylcholine, the principal chemical mediators of the parasympathetic nervous system.¹⁴ Every one of cardiology’s main drugs works on the autonomic nervous system. Their effect on plaque development is, at best, a secondary consideration.
Cardiology has the right drugs. It has the wrong explanation for why they work.
The Autonomic Model
The autonomic nervous system — the unconscious system that controls our internal organs — has two branches. The sympathetic branch drives the fight-or-flight response: adrenaline, accelerated heart rate, glucose mobilization. The parasympathetic branch, operating primarily through the vagus nerve, governs rest, digestion, and tissue repair. In a healthy person, these two branches exist in dynamic balance.
Four studies using heart-rate variability monitoring — which provides a real-time, accurate picture of autonomic balance — have shown that patients with ischemic heart disease have, on average, a reduction in parasympathetic activity of more than one-third.¹⁵ The worse the heart attack, the lower the parasympathetic activity.
Roughly 80 percent of ischemic events are preceded by chronic reductions in parasympathetic activity — brought on by smoking, emotional stress, inactivity, poor diet, hypertension, or a combination of these — followed by a sharp increase in sympathetic activity: an acute trauma, sudden exertion, or emotional shock.¹⁶
People with normal parasympathetic tone who experience a sudden sympathetic spike — a burst of intense physical activity, an emotional shock — do not have heart attacks.¹⁷ Without a preceding erosion of parasympathetic function, sympathetic activation does not cause myocardial infarction. This explains why young athletes can push their hearts to extreme limits without damage, while a sedentary, chronically stressed 55-year-old shoveling snow may die. The difference is not in their arteries. It is in the balance of their nervous system.
Women have stronger vagal (parasympathetic) activity than men, which accounts for the sex difference in heart attack incidence.¹⁸ Hypertension, smoking, diabetes, and chronic stress all suppress vagal activity.¹⁹ Every significant risk factor for heart attacks maps directly onto the autonomic nervous system. Not one maps primarily onto coronary artery plaque.
The Sequence
The actual chain of events, as documented in research by Sroka, Baroldi, and others, proceeds as follows.²⁰
Chronic reduction in parasympathetic activity degrades the heart’s baseline resilience. Then a surge in sympathetic activity — physical or emotional — floods the myocardial cells with adrenaline. This forces the cells to break down glucose through glycolysis rather than their preferred and most efficient fuel sources: ketones and fatty acids. The metabolic shift produces a dramatic increase in lactic acid within the heart cells. This happens in virtually 100 percent of myocardial infarctions.²¹ No coronary artery mechanism is required.
The lactic acid buildup creates localized acidosis, which prevents calcium from entering the cells and reduces their ability to contract. This produces the localized edema and diminished wall motion that cardiologists see on echocardiograms and stress tests — the hallmark findings of ischemic disease. If the process continues, the acidosis kills the cells. This is the tissue necrosis that defines a heart attack.
The localized edema then alters blood flow dynamics in the arteries embedded in the affected tissue, creating pressure that can rupture unstable plaques and form clots — explaining why thrombosis appears in some heart attacks but not others, and why it often develops after the event has already begun.²²
This model accounts for every observable phenomenon associated with heart disease. The coronary artery model does not.
What Has Been Built on the False Picture
Interventional cardiology — stents, bypasses, angioplasties — is a global industry measured in tens of billions of dollars annually. It rests on the three-river diagram in the cardiologist’s office. It rests on the angiogram, a test that cannot see the watershed and that systematically overestimates the blockages it can see. It rests on a theory of oxygen deprivation that measurements of oxygen during heart attacks do not support.
Meanwhile, a technology called Enhanced External Counter Pulsation (EECP) — in which inflatable cuffs on the legs and pelvis are synchronized with the heartbeat to boost venous blood flow during diastole — successfully helps more than 80 percent of patients avoid bypass surgery or stenting.²³ The treatment runs for seven weeks. It has no significant side effects. Its results last three to seven years. It works by doing what nature does: using flow to build collateral circulation.²⁴ It is a nontoxic bypass that creates the very small-vessel network that the angiogram cannot see and that the cardiologist’s diagram pretends doesn’t exist.
EECP’s success is itself a refutation of the coronary artery model. If the heart’s blood supply truly depended on three major arteries, squeezing the legs to push venous blood through the system could not possibly replace surgical grafts or metal stents in those arteries. That it does — in the majority of patients — confirms that the collateral circulation is the heart’s primary blood supply, not a backup system.
The plant medicine g-strophanthin (ouabain), derived from the Strophanthus plant, directly addresses the autonomic mechanism. It is an endogenous hormone — produced naturally in the human adrenal cortex from cholesterol — that stimulates acetylcholine production (boosting parasympathetic activity) and converts lactic acid into pyruvate, one of the heart’s preferred fuels.²⁵ It transforms the metabolic poison at the center of the heart attack cascade into a nutrient. Its production, notably, is suppressed by statin drugs — the very medications prescribed to lower the cholesterol from which the body makes its own cardiac protection.²⁶
Watershed
Giorgio Baroldi titled his major work The Etiopathogenesis of Coronary Heart Disease: A Heretical Theory Based on Morphology.²⁷ The word heretical is in the title. He knew where his evidence placed him relative to the profession.
The evidence has not been refuted. It has been ignored. The pathology studies, the failed predictions, the absent oxygen deficit, the autonomic mechanism, the collateral circulation, the success of EECP — none of this information is hidden. It exists in published studies, in books available to any physician, in video demonstrations accessible to anyone with an internet connection.
What sustains the coronary artery model is not evidence. It is the picture in the cardiologist’s office — the three neat rivers drawn by an artist, reinforced by a test that can only see those three rivers, justifying procedures that operate on those three rivers. The model is self-referencing. The test confirms the diagram. The diagram justifies the test. The procedures follow from both. And the watershed — the actual blood supply of the human heart — remains invisible at every step.
Baroldi’s images show the heart as it is. Not three rivers, but a pond. Not a plumbing problem, but a living system whose resilience is built into its structure from birth. The question is not whether the evidence supports this. The question is how long a global industry can sustain itself on a picture that isn’t real.
References
Giorgio Baroldi and Malcolm D. Silver, The Etiopathogenesis of Coronary Heart Disease: A Heretical Theory Based on Morphology (Georgetown, TX: Landes Bioscience, 2004).
Thomas Cowan, webinar, February 25, 2026; Thomas Cowan, Human Heart, Cosmic Heart (White River Junction, VT: Chelsea Green Publishing, 2016), Chapter 6.
Cowan, Human Heart, Cosmic Heart, Chapter 6. See also Knut Sroka, “On the Genesis of Myocardial Ischemia,” Zeitschrift für Kardiologie 93 (2004): 768–783.
Knut Sroka, “Heart Catheter Film,” heartattacknew.com; Sroka, “The Riddle’s Solution,” Heart Attack New Approaches.
Cowan, Human Heart, Cosmic Heart, Chapter 6; Sroka, “The Riddle’s Solution.”
Ibid.
C. S. Rihal et al., “Indications for Coronary Artery Bypass Surgery and Percutaneous Coronary Intervention in Chronic Stable Angina,” Circulation 108, no. 20 (November 2003): 2439–2445.
Cowan, Human Heart, Cosmic Heart, Chapter 6. Account of a trial reported by a cardiologist at a conference in Northern California.
W. Doerr, W. W. Höpker, and J. A. Roßner, Neues und Kritisches vom und zum Herzinfarkt (Sitzungsberichte der Heidelberger Akademie der Wissenschaften, Springer, 1975).
Baroldi and Silver, Etiopathogenesis of Coronary Heart Disease.
Ibid.; Cowan, Human Heart, Cosmic Heart, Chapter 6.
R. H. Helfant et al., “Coronary Heart Disease: Differential Hemodynamic, Metabolic and Electrocardiographic Effects in Subjects with and without Angina during Atrial Pacing,” Circulation 42, no. 4 (October 1970): 601–610.
Cowan, Human Heart, Cosmic Heart, Chapter 7.
Ibid.
Baroldi and Silver, Etiopathogenesis of Coronary Heart Disease; Sroka, “On the Genesis of Myocardial Ischemia.”
B. Takase et al., “Heart Rate Variability in Patients with Diabetes Mellitus, Ischemic Heart Disease and Congestive Heart Failure,” Journal of Electrocardiology 25, no. 2 (April 1992): 79–88.
Sroka, “On the Genesis of Myocardial Ischemia.”
Knut Sroka et al., “Heart Rate Variability in Myocardial Ischemia during Daily Life,” Journal of Electrocardiology 30, no. 1 (January 1997): 45–56.
Sroka, “On the Genesis of Myocardial Ischemia.”
Ibid.; Baroldi and Silver, Etiopathogenesis of Coronary Heart Disease.
James Scheuer and Norman Brachfeld, “Coronary Insufficiency: Relations between Hemodynamic, Electrical, and Biochemical Parameters,” Circulation Research (1966): 178–189.
Cowan, Human Heart, Cosmic Heart, Chapter 7.
Debra Braverman, Heal Your Heart with EECP (Berkeley, CA: Celestial Arts, 2005).
Ibid.
H. Fürstenwerth, “Ouabain — the Insulin of the Heart,” The International Journal of Clinical Practice 64, no. 12 (November 2010): 1591–1594; H. Fürstenwerth, “On the Differences between Ouabain and Digitalis Glycosides,” American Journal of Therapeutics 21, no. 1 (January–February 2014): 35–42.
Cowan, Human Heart, Cosmic Heart, Chapter 7.
Baroldi and Silver, Etiopathogenesis of Coronary Heart Disease.
New Biology Clinic
For those of you looking for practitioners who actually understand terrain medicine and the principles we explore here, I want to share something valuable. Dr. Tom Cowan—whose books and podcasts have shaped much of my own thinking about health—has created the New Biology Clinic, a virtual practice staffed by wellness specialists who operate from the same foundational understanding. This isn’t about symptom suppression or the conventional model. It’s about personalized guidance rooted in how living systems actually work. The clinic offers individual and family memberships that include not just private consults, but group sessions covering movement, nutrition, breathwork, biofield tuning, and more. Everything is virtual, making it accessible wherever you are. If you’ve been searching for practitioners who won’t look at you blankly when you mention structured water or the importance of the extracellular matrix, this is worth exploring. Use discount code “Unbekoming” to get $100 off the member activation fee. You can learn more and sign up at newbiologyclinic.com
I had my first stent, almost 20 years ago in the OM artery. It did result in a vast improvement in my main symptom, which was shortness of breath.
I had to have two more stents put in the same artery about five years later,and again, my symptoms improved.
Because I refuse to take all of the crappy medicines that they wanted me to take, especially statins, my doctor, as a last resort, let me try the EECP and the results were amazing!
I have been virtually symptom-free for the last five years. I was able to stop taking all nitrates which I was using when I had an issue with my breath.
I am 75 years old now and my cardiologist doesn’t understand why I’m doing so well. He told me I was gonna live to 90 and then at my last visit upgraded that to 100!
I think the EECP is very little known and should be used much more widely, but then a lot of people would rather take a pill then go through a rigorous seven week treatment. I also suspect that the drug companies prefer it that way!
I like the idea of EECP it fits nicely with the benefits of Blood flow Restriction which both my husband and I find very helpful. Since I’ve been using this method every day, I no longer bruise easily, don’t get up to pee in the night (previously it was at least twice) and have more energy and better sleep quality. I would also highly recommend reading Tom Cowan’s book because it’s both useful and fascinating. The essay discusses the implications of both stress and emotional upset on cause of heart attacks. Chinese medicine has long been aware of these links, there is even some research on changes to daylight saving causing an increase in heart attacks when the clocks go forward.