
The Final Pandemic
By Drs Mark & Samantha Bailey – Unbekoming Book Summary


The medical establishment has become a major threat to health…Medicine is about to become a prime target for political action that aims at an inversion of industrial society. — Ivan Illich, Medical Nemesis, 1975.
I’ve had The Final Pandemic on my to read list for a while, and then Dr Judy Wilyman, during our interview tipped me over the edge and got me to pay attention to it.
Interview with Judy Wilyman PhD - Lies are Unbekoming (substack.com)
11. Some of your recent writing has alleged fraud and deception by pharmaceutical companies and regulators in relation to COVID vaccines. Can you summarize the evidence you believe supports these claims?
The evidence for the medical fraud that has led to government tyranny and totalitarianism is described in my article, ‘Creating a Global Pandemic’, published in The Master of Health Magazine in 2020, and ‘The Final Pandemic: An Antidote to Medical Tyranny’ by Dr. Mark and Sam Bailey
It’s a magnificent book in that it’s easy to read, it’s short and its goal is to help the curious layperson come to terms with the history of untruths that have been used to create the most recent “pandemic” but more importantly to understand the basis of the biosecurity state that has come out of the shadows ready to rule us.
Auditing virology is no trivial matter. It does matter, a lot, whether it’s fundamentally and functionally true or not.
It also matters whether it is a fact based science or a faith based pseudoscience.
I highly recommend the book, and I especially recommend it as a tool that will help others.
With thanks to Drs Samantha and Mark Bailey.
The Final Pandemic
An Antidote to Medical Tyranny
By Drs Mark & Samantha Bailey – Unbekoming Book Summary
The Final Pandemic - Dr Sam Bailey
Foreword by Prof. Tim Noakes
“Moral courage is a rarer commodity than bravery in battle or great intelligence. Yet it is the one essential, vital quality for those who seek to change a world that yields most painfully to change.” — Robert Kennedy Snr., 1966.
The book you are holding has been written by two of the most morally courageous physicians on our planet. Why so?
Because they are truth seekers whose conscience does not allow them to remain silent about that which they believe to be untrue, regardless of any unwelcome consequences their principled stance has and will have for their social lives and professional careers. For what they conceive to be the great untruth is nothing less than the most important global medical event of the past 100 years, perhaps ever – the COVID-19 pandemic caused by the SARS-CoV-2 virus.
The narrative untruth with which they disagree runs something like this: Beginning in January 2020 the world’s most trusted news agencies began to inform the world that a deadly novel virus – SARS-CoV-2 – was on the loose, certain to kill millions across the globe in just a few months. But that was not all. Later we were warned that this virus was just the first of many yet to come. To be followed in 2025 by the even more scary sounding- Severe Epidemic Enterovirus Respiratory Syndrome (SEERS) - according to one simulated pandemic preparedness exercise.
These deadly viruses, we are told, exist, hidden, in animal reservoirs across the globe, any of which can ignite a global pandemic at any moment, simply by infecting a single human with whom any might come into contact (see Ch. 2 - Scapegoats for Disease). Not currently explained though, is why this novel form of disease transmission has surfaced only quite recently, given that our immediate human ancestors have lived in close proximity with these potential animal hosts for centuries.
Once the virus escapes from inside the cells of an animal host, transferring itself into the susceptible organs of that first human contact – now known as ‘Patient Zero’ – it begins to multiply, rapidly producing millions of identical copies of itself. Unwittingly, but very rapidly, Patient Zero then transfers the virus to all humans with whom he or she is in contact. Conveyed by international air travel and abetted by its very high infectivity, the virus then rapidly circles the globe, igniting a global catastrophe of biblical proportions.
Faced with this inevitability, the responsibility of all governments concerned about their peoples’ health, is immediately to protect every individual on the planet “for the greater good” since, “no one is safe until all are safe”.
Thus the need for an immediate, carefully co-ordinated, uniform global response that includes restricting everyone’s movements to only those that are absolutely essential; wearing face masks in public; and the development of “safe and effective” vaccines that protect against illness whilst blocking any further spread of the virus. In this way the pandemic is brought under control, quickly, safely and effectively, with a minimum loss of life and without imposing an intolerable financial burden on anyone.
But what if all this narrative is just a contrived fiction?
That is a question with which the authors of this book have been grappling for some time. Here they present a concise summary of the most compelling evidence that their search for truth has uncovered.
In this exhaustively researched and carefully documented book they throughly eviscerate that official narrative, not least by exposing a series of basic, indeed elementary, scientific “errors” without which the narrative has no foundation. They also explain how this fake narrative was sold to the world by the compliant and incentivized mainstream media aided by a subservient and well-rewarded medical profession.
The First Error: The method used by virologists to detect the presence of a virus is indirect, unscientific and essentially unproven, not least because it fails to incorporate appropriate experimental controls (as is required in all scientific experimentation).
The official pandemic narrative requires the presence of a pathogenic virus able to transfer itself without difficulty, first from its host animal to Patient Zero and then from Patient Zero to the rest of humanity. For without a virus there can be no viral pandemic.
The challenge for all those who study viruses, is that unlike other alleged infectious agents claimed to cause human disease including bacteria, fungi, protozoa, and helminths (worms), viruses are tiny, very shy creatures that dislike being seen and are reluctant to replicate in laboratories in the presence of prying humans. So scientists have had to invent a complicated process to identify their presence.
In this process they developed what is considered the gold standard test but which is based on a circular logic that becomes infinitely self-fulfilling (see Figure 1).
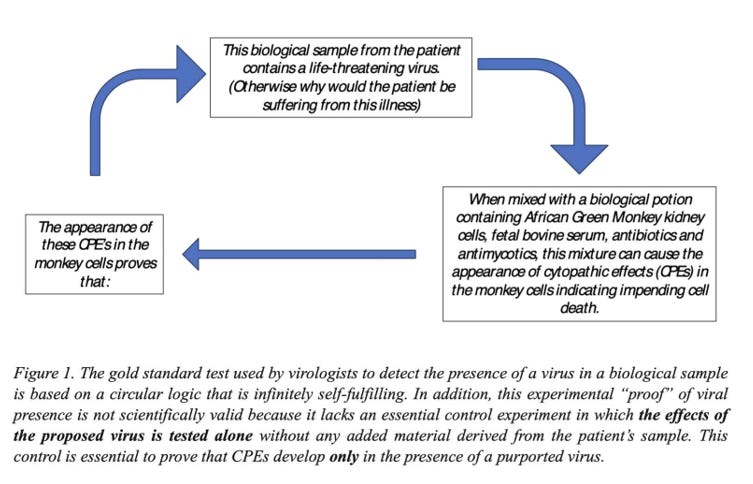
The circular logic begins with the virologist’s certainty that the sample taken from an ill patient must contain a virus so that any other possible causes of the illness can be ignored. The patient’s sample is then mixed with a solution containing a multitude of cells and chemicals. If, after a few days the kidney cells show histological evidence of cell death (cytopathic effects - CPEs), it is concluded that a cytopathic virus, present in the patient’s sample, is the cause.
But this is not how proper science is conducted.
For this false experimental method cannot exclude the alternative explanation that something other than an unseen virus caused the observed CPEs. This possibility can only be excluded with an experimental control in which the biological potion contains everything but the patient’s alleged viruses. If this control experiment does not produce CPEs, then it is reasonable to conclude that a cytopathic agent was present in the patient’s sample (although it would still not be definitive evidence that this was the cause of the patient’s presentation).
The authors are not the first to criticize the absence of the experimental control; it is clearly described by Dr Stefan Lanka who argues that in the original description of this experimental method, “no control experiments were performed to exclude the possibility that it was the deprivation of nutrients as well as the antibiotics which led to the cytopathic effects.”7 Indeed those who described this novel method noted that many cells also died without being treated with the “infectious” sample. To hide this inconvenient finding, they conveniently concluded that this effect must have been due to the presence of unknown viruses or other factors in the biological potion. This logic is also counter-scientific since it assumes that the outcome of the experiment is already known even before the experiment begins.
But the criticism does not end there. For the authors ask the seemingly obvious question: Since COVID-19 is a human respiratory disease, not a monkey kidney disease, why is it necessary to use monkey kidney cells to detect a viral presence? Especially when kidney cells, “are designed to process mostly sterile blood, not deal with respiratory secretions and all kinds of inhaled particles” (see Ch. 4 - How to Create ‘Virus Genomes’). The probable answer is that the use of any other cell lines fails to produce the CPEs that are so readily observed when monkey kidney cells are used. Thus other cell lines are unable to “detect” a viral presence with the same certainty as the monkey kidney cells.
The authors wonder why these scientists were not more interested in developing methods to provide direct proof of viral presence.
But there is a simple experiment to document the true precision of this gold standard CPE test. Perform “blinded” tests in certified laboratories by supplying the experts with patient samples without providing any prior information of what the expected results might be. The most important test would be one from a healthy patient in whom there is no likelihood that a life-threatening virus is present. If the experts return a positive viral test, the story ends. If not, the virologists would still need to demonstrate that their in vitro (laboratory) cell culture experiments correspond to in vivo (living organism) reality. This would include the true physical isolation of the alleged virus particles and subsequent clinical experiments to establish their capacity to cause disease.
The Second Error: The method for detecting the genome of the virus does not require that the sample to be tested comes from an isolated (i.e. purified) virus. Instead it is a computer-generated “best guess” genome pieced together from millions of different genetic sequences present in a biological potion.
Once the presence of CPEs in an initial test has “proven” the presence of an infectious virus in the tested patient, the next step is to isolate a virus particle and extract its genetic structure. But here too there is a significant problem. For the biological potion in which the virus is supposedly “isolated” contains a mass of genetic information and only a tiny section will have come from any alleged virus. To overcome this problem, the scientists came up with another unique solution.
Their solution (see Ch. 4 - How to Create ‘Virus Genomes’) involves the use of specific computer software to re-splice all the genetic material present in the biological potion to produce a product that has the appearance of an isolated viral genome. This process is itself dependent on the existence of a library of viral genomes, all produced by exactly the same methods.
But even if this method does indeed identify a real viral genome, this identification can never prove that: (a) the identified virus is the cause of the patient’s (especially Patient Zero’s) illness or that, (b) the virus so identified is contagious and transferable and has the capacity to generate the pandemic. As it stands, it has not yet been possible to isolate, purify and describe the complete viral genome from virus particles isolated from a living patient infected with a rapidly-replicating, life-threatening virus. See for example the surprising outcome of the unsuccessful attempts to isolate the measles virus, described in the section Don’t Worry if the Germ Even Exists (Ch. 3). The authors have indeed, as they say, “opened the door into the world of ‘viral genomes’ and how they are created, without any proof that the genetic material comes from a virus”.
The Third Error: The pandemic was not a viral pandemic. It was a testing pandemic driven by the false interpretation of Polymerase Chain Reaction (PCR) tests which have little or no relevance to the practice of clinical medicine.
Clinical medicine of the kind that the authors and I were taught in our medical training is based on an historic approach in which the medical diagnosis is made only when the following steps are properly and judiciously enacted:
1. The medical practitioner takes an extensive medical history from the ill patient.
2. The medical practitioner performs a relevant medical examination of the ill patient.
3. On the basis of 1 and 2, the medical practitioner draws up a differential diagnosis of all the conditions that could possibly be causing the patient’s ill health.
4. The medical practitioner requests whichever special investigations like blood tests and imaging techniques that will help eliminate all but one of the conditions considered in the differential diagnosis.
5. The medical practitioner draws up a treatment protocol based on the most probable diagnosis.
6. The medical practitioner monitors the patient’s response to the treatment protocol and makes the necessary therapeutic adjustments as required.
The key point is that once the COVID-19 pandemic was declared, this venerated medical approach honed over centuries, was hastily abandoned at least as it applied to patients presenting with any flu-like illness that might be COVID-19 at the time or since.
Instead the only diagnostic step now considered necessary to make the diagnosis is a “test” (Step 4), even in the absence of illness. Instantly it has become acceptable to believe that a single biological test replaces any need for the medical practitioner to perform a proper medical examination.
Thus on the 7th of August, 2020, the World Health Organization (WHO) declared that a confirmed case of COVID-19 infection was one in which there was “laboratory confirmation of COVID-19 infection, irrespective of clinical signs and symptoms” (see Ch. 1 - Meaningless Cases). In other words, a perfectly healthy person could now be declared ill if he or she had “laboratory confirmation of COVID-19 infection” and without the need for a proper medical examination, which is the time-honored way by which the medical practitioner arrives at a plausible differential diagnosis.
Of course if the patient is perfectly healthy, there is no need for a differential diagnosis.
So quite conveniently for the nefarious goals of the WHO, this novel definition of illness introduced the (unproven) concept of the asymptomatic COVID-19 carrier who could spread infection without showing any evidence of the illness. Or the even more fear-inducing “superspreader,” first introduced to the world through the possibly fictitious early 1900s tale, described in ‘Typhoid Mary’ - The Original “Superspreader” Story (Ch. 1). Naturally if asymptomatic “superspreaders” exist then everyone must be tested regularly to ensure that the uninfected are not exposed unwittingly to the virus. This then set the stage for a pandemic of universal testing for the presence of COVID-19 in the perfectly healthy.
But the two tests used for this laboratory confirmation - the Polymerase Chain Reaction (PCR) test (see Ch. 4 - What is the Polymerase Chain Reaction?) and the Lateral Flow or Rapid Antigen Test – are chemical tools designed for the sole purpose of detecting the presence of a minute number of target molecules that are considered to be present in the purported SARS-CoV-2 virus. That is all the PCR test can detect; it can detect the presence of a tiny number of molecules that may or may not have any relationship to an infecting “virus”.
So powerful in fact is the process that according to the inventor of the methodology, Kary Mullis: “PCR is just a process that allows you to make a whole lot of something out of something. It doesn’t tell you that you are sick, or that the thing that you ended up with was going to hurt you or anything like that.” This would explain why Tanzanian President John Mogufuli was able to return positive COVID-19 tests from a papaya, a quail and a goat, although all were reportedly asymptomatic.
As the authors describe: “despite the incredible achievement and development of the PCR, along with technical improvements over the decades, the nature of what the PCR can do has not changed: it simply amplifies selected target genetic sequences. It cannot confirm where the genetic material came from, whether it came from an intact organism, or whether a human is ‘infected’ by something.” So the COVID-19 pandemic was based on a test that cannot differentiate between a sample coming from an Olympic athlete in the peak of health. Or from someone who has been dead and buried, already for 100 years.
And it was on the basis of this test that the world was locked down.
The Fourth Error: Viral contagion – that is the passage of a virus from the cells of one human to another, or from the host animal to Patient Zero – has yet to be properly documented.
From childhood we are taught to believe in the germ theory; which is the basis for the modern COVID-19 narrative. In the past we had no reason to question it because it was so obviously true. We all know that as children we caught our colds or our single bout of measles or chickenpox from the infected child in our school classroom. But here we again learn that the basis for that accepted truth is perhaps less robust than the mainstream is prepared to admit.
For example the most lethal pandemic of the recent past was the Spanish Flu of 1918. Less well known is that experiments were conducted to determine if a contagious agent could be identified as the sole cause of the pandemic in sick patients. But these attempts universally failed even though the researchers went to extraordinary lengths, perhaps considered unethical by modern medical standards (see Ch. 3 - What Human-to-Human Transmission?) to establish the presence of a transmissible agent.
So whatever killed more than 21 million humans around the world in the 1918 Spanish Flu Pandemic, it was never shown to be a transmissible infectious agent. Indeed the person in charge of this research, Dr Milton Rosenau, would later write: “As a matter of fact, we entered the outbreak with a notion that we knew the cause of disease, and were quite sure we knew how it was transmitted from person to person. Perhaps, if we had learned anything, it is that we are not quite sure what we know about the disease.”
But this is not the sole example of discoveries that question the medical certainty about the cause of these “infectious” diseases and how they are transmitted. Here the authors draw attention to the continuing but seldom acknowledged doubts about the origins and causes of the common cold, polio, rabies and measles (Ch. 3); whooping cough (Ch. 4); HIV/AIDS (Ch. 5); and the clear evidence that deaths from the childhood “infectious diseases” had almost disappeared well before the advent of specific vaccines for each of these conditions (various graphs courtesy of Dissolving Illusions). Finally, they present the equally inconvenient evidence that vaccinated children are generally less healthy than their non-vaccinated peers (see Ch. 6 - What are Vaccines Doing?).
Summary and Final Piece of Evidence
The timeless value of this book is that it presents, in the purest, most direct and honest way, the most convincing evidence why the COVID-19 pandemic was based on a fictional science that has its origins at least a century ago with the earliest, essentially primitive attempts to develop vaccines to prevent viral illnesses.
I suggest that if the evidence the authors have presented, was ever examined in a court of law before a panel of independent thinkers to evaluate the efficacy of vaccinations including the global response to the COVID-19 pandemic, those independents would have to come to one conclusion, namely, that the evidence the authors have presented here is quite simply, irrefutable, however alarming that conclusion might be.
But there is one final body of evidence that confirms the veracity of the authors’ overarching theme. Keeping in mind that they begin their book with a section entitled Allopathic Medicine Invents Diseases, here is the time line for the development of the “science” relating to the novel SARS-CoV-2 pandemic:
Day 1 30th of December, 2019
“An eye doctor in China spots a case of supposedly atypical pneumonia.”
Day 7 5th of January, 2020
The World Health Organization (WHO) announces they have identified 44 cases of atypical pneumonia of unknown aetiology (APOUA) in a specific population of 8 million people in China.
Day 9 7th of January, 2020
The WHO announces that the APOUA is caused by a novel SARS-like virus.
Day 12 10th of January, 2020
The firm manufacturing the first COVID-19 PCR tests [Olfert Landt’s TIB Molbiol] starts shipping them. The first “viral genome” for SARS-CoV-2 is published.
Day 14 12th of January, 2020*
The WHO accepts Professor Christian Drosten’s PCR testing protocol as, “the gold standard for the testing for this novel disease”.
Day 23 21st of January, 2020
The Drosten/Landt PCR testing protocol is submitted for review to an international scientific publication.
Day 25 23rd of January, 2020
The paper describing the Drosten/Landt PCR testing protocol is accepted for publication and is published within 27 hours in a journal of which Drosten is an editor.
Day 26. 24th of January, 2020
A paper describing the clinical features of COVID-19 is published by Chinese scientists in The Lancet.
Day 32 30th of January, 2020
The first letter describing asymptomatic transmission of COVID-19 is published in The New England Journal of Medicine.
One might perhaps conclude that requiring just 32 days to identify and fully describe a novel infectious disease including the genome of the causative agent, whilst also discovering that it can be transmitted by persons without any symptoms of illness, is perhaps just too good to be true.
A Final Word
I began the foreword with a quote from Robert Kennedy Snr’s Ripples of Hope speech delivered at my Alma Mater in June 1966. The speech includes another quote relevant to this book, its authors and our modern predicament:
Each time a man stands up for an ideal, or acts to improve the lot of others, or strikes out against injustice, he sends forth a tiny ripple of hope, and crossing each other from a million different centers of energy and daring those ripples build a current which can sweep down the mightiest walls of oppression and resistance.
This book is not the first to expose the false science behind the popular virus and vaccination narratives in general, or those that have sustained the COVID-19 pandemic in particular; but it may just be one of the very best.
Our collective hope must be that when those who read this book truly understand what is the truth and how we have been willfully misled, with catastrophic consequences, their ripples of frustration will coalesce into a giant current sweeping all before it, igniting a global demand for answers from those in government, in politics, in medicine and in science, indeed, from all who are ultimately accountable for their part in the dishonesty of what has happened.
And that this new knowledge will ensure that we, the public, never, ever allow something similar to be repeated.
Prof. Timothy D. Noakes OMS, MB ChB, MD, DSc, PhD (hc), FACSM, (hc) FFSEM(UK), (hc) FFSEM(Ire)
35 Questions & Answers
Question 1: What is the central premise of "The Final Pandemic" and how does it challenge conventional beliefs about infectious diseases?
The central premise of "The Final Pandemic" is that the concept of contagious and death-dealing 'germs' is finished. The book challenges conventional beliefs about infectious diseases by arguing that there is no scientific evidence for germ theory, viruses, or the transmission of diseases between humans. It posits that alleged pandemics are manufactured crises, created through misleading case definitions, unreliable testing methods, and media manipulation rather than actual new diseases or pathogens.
Question 2: How do the authors define 'allopathic medicine' and what criticisms do they present about this approach?
The authors define allopathic medicine as a system where 'illness' may or may not have symptoms and where 'disease' may or may not come with any actual dis-ease. They criticize this approach for inventing diseases to suit its purposes, manipulating disease classifications, and creating fictional diseases for the benefit of the medico-pharmaceutical industry. The authors argue that allopathic medicine focuses on treating symptoms rather than addressing underlying causes, leading to unnecessary interventions and potential harm to patients.
Question 3: What role did the PCR test play in the COVID-19 pandemic according to the authors?
According to the authors, the PCR test played a central role in manufacturing the appearance of a COVID-19 pandemic. They argue that the PCR is not a diagnostic tool but a manufacturing technique for molecular amplification. The authors claim that the test's high sensitivity led to the detection of genetic sequences that were incorrectly interpreted as evidence of a virus, resulting in false positives and inflated case numbers. They assert that the pandemic was essentially a "testing pandemic" rather than a viral one.
Typhoid Mary:
The book discusses 'Typhoid Mary' (Mary Mallon) as an example of how the concept of asymptomatic carriers and superspreaders was historically constructed. The authors argue that there was no scientific evidence that Mary Mallon actually spread typhoid fever. They point out that the diagnosis of typhoid fever was based on subjective symptoms and that no proper isolation of the supposed causative agent, Salmonella typhi, was ever performed.
The authors use this case to illustrate how the germ theory paradigm creates narratives around disease transmission without solid scientific evidence. They suggest that factors such as poor hygiene or food contamination could explain disease clusters, rather than the idea of a single asymptomatic carrier spreading illness.
Question 4: How do the authors explain the concept of 'zoonosis' and what criticisms do they present about it?
The authors describe zoonosis as the unproven theory that diseases jump from animals into humans. They criticize this concept as lacking scientific evidence and being used to create fear-inducing headlines. The authors argue that claims about zoonotic threats are often made without proper scientific basis and are used to justify unnecessary interventions and funding for research. They suggest that environmental and nutritional factors are more likely causes of disease than animal-to-human transmission of pathogens.
Question 5: What historical examples do the authors use to challenge the idea of human-to-human disease transmission?
The authors use several historical examples to challenge the idea of human-to-human disease transmission. A key example is the 1918 Spanish Flu experiments conducted by Dr. Milton Rosenau, where volunteers were exposed to bodily fluids from sick patients in various ways, yet none became ill. They also discuss the Common Cold Unit's experiments, which failed to demonstrate that viruses were causing colds in human volunteers. These examples are used to argue that the concept of contagious diseases lacks scientific evidence.
Question 6: How do the authors describe the process of creating "virus genomes" and what criticisms do they present?
The authors describe the process of creating "virus genomes" as a computer-based method that assembles genetic sequences from mixed samples without isolating an actual virus. They criticize this approach, arguing that it relies on circular reasoning and unproven assumptions. The authors claim that virologists use genetic material from various sources, including human cells and contaminants, to create hypothetical viral genomes. They argue that this process does not prove the existence of a virus or its role in causing disease.
Ebola:
The book challenges the mainstream narrative about Ebola as a highly infectious and deadly virus. The authors argue that despite alarming claims about its contagiousness, Ebola has never spread significantly outside of poor African countries. They point out that even in cases where individuals supposedly infected with Ebola traveled to other countries, no widespread outbreaks occurred.
The authors suggest that the symptoms attributed to Ebola could be explained by other factors such as malnutrition, poor sanitation, and exposure to environmental toxins. They criticize the lack of proper isolation and characterization of the alleged Ebola virus, arguing that the diagnostic methods used (like PCR tests) are not reliable for identifying a specific pathogen or diagnosing a disease.
Question 7: What is the significance of the 'cytopathic effect' (CPE) in virology?
The cytopathic effect (CPE) is mistakenly used in virology as evidence of viral presence and infection. They argue that CPEs are simply the abnormal appearances of stressed cells breaking down and dying, which can occur due to various factors unrelated to viruses. The authors contend that virologists incorrectly interpret these cellular changes as proof of viral infection, ignoring other potential causes such as the toxic effects of antibiotics or other substances used in cell cultures.
Question 8: How do the authors explain the decline in mortality rates of common diseases before the introduction of vaccines?
The authors argue that the decline in mortality rates of common diseases occurred primarily due to improvements in living standards, nutrition, and sanitation, rather than medical interventions or vaccines. They present historical data showing significant reductions in disease mortality before the widespread use of vaccines. The authors contend that this evidence challenges the claim that vaccines were responsible for conquering these diseases and suggest that the role of vaccines in public health has been overstated.
Question 9: What criticisms do the authors present regarding the development and testing of vaccines?
The authors criticize vaccine development and testing on several fronts. They argue that the underlying premise of vaccines is flawed due to the lack of evidence for germ theory and viral causation of diseases. They question the scientific validity of animal studies used in vaccine research and criticize the lack of proper control groups in many vaccine trials. The authors also raise concerns about the potential harm caused by vaccines, citing increases in allergic and inflammatory conditions in children following the expansion of childhood vaccination schedules.
Rosenau:
Dr. Milton Rosenau's experiments in 1918 during the Spanish Flu pandemic are prominently featured in the book as evidence against the idea of human-to-human disease transmission. The authors describe how Rosenau and his team conducted experiments where they attempted to infect healthy volunteers with influenza using various methods, including exposing them to bodily fluids from sick patients and having them interact closely with ill individuals.
Despite these efforts, none of the volunteers became ill, which the authors present as a significant challenge to the concept of contagious diseases. They argue that this pivotal research has been largely ignored by the medical establishment because it contradicts the germ theory paradigm. The book suggests that Rosenau's own conclusion - that they were not quite sure what they knew about the disease - should have led to a reevaluation of the infectious disease model.
Question 10: How do the authors describe the role of the World Health Organization (WHO) in global health policy?
The authors portray the World Health Organization (WHO) as an influential body that promotes and sustains the germ theory paradigm and vaccine agenda. They argue that the WHO's declarations, such as pandemic announcements, trigger global responses without sufficient scientific basis. The authors suggest that the WHO is heavily influenced by private interests, particularly through funding from entities like the Bill & Melinda Gates Foundation. They criticize the organization for its role in shaping global health policies that benefit the pharmaceutical industry rather than public health.
Question 11: What is the authors' perspective on the influence of the Bill & Melinda Gates Foundation in global health?
The authors view the Bill & Melinda Gates Foundation as having an outsized and concerning influence on global health policy. They highlight the foundation's significant financial contributions to organizations like the WHO, GAVI, and various research institutions. The authors argue that this funding allows Gates to steer global health initiatives towards vaccination programs and other interventions that benefit the pharmaceutical industry. They suggest that this influence extends to shaping media narratives about health issues through grants to various news outlets and academic journals.
Question 12: How do the authors explain the concept of 'asymptomatic transmission' in relation to infectious diseases?
The authors regard the concept of 'asymptomatic transmission' as a flawed idea used to justify widespread testing and interventions. They argue that this concept was introduced to explain the lack of visible illness in many people who tested positive for COVID-19. The authors contend that asymptomatic transmission is not scientifically proven and is used to maintain the illusion of a spreading pandemic even when people are not visibly sick. They suggest that this concept contradicts traditional understandings of disease and is used to expand the reach of medical interventions.
Common Cold Unit:
The book discusses the Common Cold Unit (CCU) that operated in the UK from 1946 to 1989, criticizing its methods and conclusions. The authors argue that despite decades of research, the CCU failed to demonstrate that viruses cause the common cold or that colds are transmissible between humans. They point out that even when the unit claimed to have "isolated" coronaviruses, they were actually observing cellular breakdown in artificial lab conditions, not proving the existence of a virus.
The authors suggest that the CCU's experiments, which often involved subjecting volunteers to stressful conditions, demonstrate that factors other than viruses could be responsible for cold symptoms. They argue that the unit's failure to develop a cure or vaccine for the common cold, despite years of research, further undermines the viral theory of colds.
Question 13: What criticisms do the authors present regarding the use of animal studies in virus research?
The authors strongly criticize the use of animal studies in virus research, describing them as cruel and scientifically invalid. They argue that these experiments, such as injecting concentrated substances directly into animals' lungs or brains, do not replicate natural disease processes. The authors contend that the results of such studies are misinterpreted to support pre-existing beliefs about viral transmission and pathogenicity. They suggest that these experiments cause unnecessary animal suffering without providing reliable or relevant information about human diseases.
Question 14: How do the authors describe the role of the media in shaping public perception of pandemics?
The authors portray the media as a key player in manufacturing pandemic narratives. They argue that mainstream media outlets uncritically promote fear-inducing stories about new diseases without proper scientific scrutiny. The authors highlight how media coverage often focuses on dramatic individual cases or misleading statistics to create a sense of widespread danger. They also discuss the media's role in suppressing alternative viewpoints and promoting official narratives, particularly during the COVID-19 pandemic.
Question 15: What is the authors' perspective on the concept of 'herd immunity' through vaccination?
The authors reject the concept of 'herd immunity' through vaccination as scientifically unfounded. They argue that this idea is based on the unproven assumptions of germ theory and vaccine efficacy. The authors contend that there is no reliable evidence showing that mass vaccination programs provide community-wide protection against diseases. Instead, they suggest that true health is achieved through proper nutrition, sanitation, and addressing environmental factors, rather than through artificial immune stimulation via vaccines.
Pellagra:
The book uses pellagra as an example of how nutritional deficiencies have been mistakenly attributed to infectious causes. The authors describe how pellagra, now known to be caused by niacin deficiency, was once thought to be an infectious disease. They detail how researchers in the early 20th century, influenced by germ theory, searched for a microbial cause and even claimed to have isolated bacteria responsible for the condition.
The authors argue that the eventual recognition of pellagra as a nutritional deficiency disease should have led to a broader reevaluation of the germ theory paradigm. They use this historical example to suggest that many other conditions attributed to pathogens might actually be the result of nutritional or environmental factors.
Question 16: How do the authors explain the historical development of germ theory?
The authors portray the historical development of germ theory as a misguided turn in medical science, primarily driven by Louis Pasteur and Robert Koch in the late 1800s. They argue that despite inconsistencies and failures in their theories and treatments, Pasteur and Koch's influence became pervasive. The authors contend that this led to a reductionist "one disease—one cause (pathogen)—one miracle cure" model, which they claim has resulted in repeated failures. They suggest that this paradigm shift allowed the pharmaceutical industry to gain significant power and influence over public health policy.
Question 17: What criticisms do the authors present regarding the isolation and purification of viruses?
The authors argue that there is no scientific evidence of viruses being physically isolated and purified from any tissues or bodily fluids of sick humans or animals. They criticize virologists for abandoning direct isolation attempts and instead relying on indirect methods such as observing cytopathic effects in cell cultures. The authors contend that what virologists call "isolation" is actually a process of mixing various substances together, rather than separating a specific particle. They argue that this lack of true isolation undermines the entire basis of virology.
Question 18: How do the authors describe the relationship between the pharmaceutical industry and medical research?
The authors portray the relationship between the pharmaceutical industry and medical research as deeply problematic and riddled with conflicts of interest. They argue that the industry exerts significant control over the direction and interpretation of research, often to promote their products rather than improve public health. The authors highlight how funding from pharmaceutical companies influences study designs, data interpretation, and publication of results. They suggest that this relationship has led to a bias towards drug-based interventions and away from investigating underlying causes of disease.
Polio:
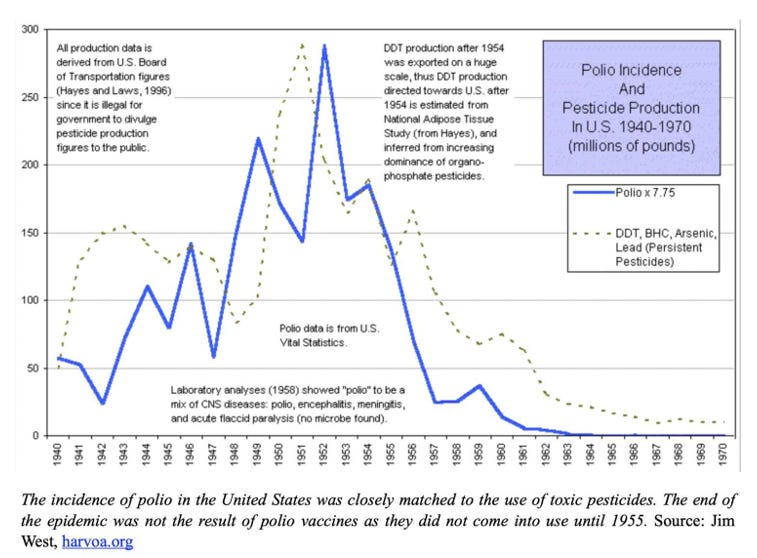
The book presents a controversial perspective on polio, arguing that it was not caused by a virus but was instead the result of environmental toxins, particularly pesticides like DDT. The authors claim that the rise and fall of polio cases correlate strongly with the use of these chemicals, rather than with the introduction of vaccines.
They criticize the conventional narrative about polio vaccines, arguing that the decline in polio cases was already underway before mass vaccination began. The book suggests that changes in diagnostic criteria and the reclassification of polio-like symptoms under different names contributed to the apparent success of the vaccine. The authors use polio as an example of how environmental causes of disease are often overlooked in favor of the germ theory model.
Question 19: What is the authors' perspective on the concept of 'emerging infectious diseases'?
The authors view the concept of 'emerging infectious diseases' as a manufactured threat used to justify ongoing funding and interventions by the medical establishment. They argue that claims about new pathogens emerging from nature or through zoonotic transmission lack scientific basis. Instead, the authors suggest that apparent disease clusters or new syndromes are often the result of environmental factors, toxins, or changes in diagnostic criteria. They contend that the focus on 'emerging infectious diseases' distracts from addressing the real causes of ill health.
Question 20: How do the authors explain the role of environmental factors in disease causation?
The authors emphasize the importance of environmental factors in disease causation, contrasting this with the germ theory approach. They argue that many conditions attributed to infectious agents are actually the result of toxins, nutritional deficiencies, or other environmental stressors. For example, they link the rise of polio to increased use of pesticides like DDT. The authors contend that focusing on these environmental factors would lead to more effective prevention and treatment strategies than the current emphasis on fighting alleged pathogens.
Question 21: What criticisms do the authors present regarding the use of mathematical modeling in epidemiology?
The authors criticize the use of mathematical modeling in epidemiology as misleading and potentially harmful. They argue that these models, such as those used during the COVID-19 pandemic, often rely on flawed assumptions and incomplete data. The authors point to examples like Neil Ferguson's predictions, which they claim were grossly inaccurate but still used to justify severe interventions like lockdowns. They suggest that these models are more about creating alarming scenarios to drive policy decisions than accurately predicting disease spread.
Rabies:
The book challenges the conventional understanding of rabies as a viral disease. The authors argue that there is no scientific evidence of a rabies virus being isolated and proven to cause the condition known as rabies. They criticize Louis Pasteur's work on rabies vaccines, suggesting that his claimed successes were fraudulent and that his treatments may have actually caused harm.
The authors point out the rarity of rabies cases and question the need for widespread rabies vaccination programs. They suggest that symptoms attributed to rabies could have other causes and that the fear surrounding the disease is disproportionate to its actual occurrence. The book uses rabies as an example of how unproven theories about viral diseases can lead to unnecessary and potentially harmful medical interventions.
Question 22: How do the authors describe the process of vaccine development and approval?
The authors portray vaccine development and approval as a rushed and scientifically questionable process, particularly in the context of the COVID-19 pandemic. They argue that the traditional safeguards and long-term studies were bypassed in favor of rapid deployment. The authors criticize the use of emergency use authorizations and the lack of proper control groups in vaccine trials. They suggest that the process is driven more by political and economic interests than by genuine concern for public health and safety.
Question 23: What is the authors' perspective on the concept of 'gain-of-function' research?
The authors view 'gain-of-function' research as a dangerous and misguided endeavor. They argue that claims about creating more dangerous versions of viruses through this research are based on flawed premises, given their stance that pathogenic viruses have not been proven to exist. The authors suggest that experiments described as 'gain-of-function' research often involve introducing toxic substances to animals or cell cultures, misinterpreting the results as evidence of enhanced viral pathogenicity. They contend that this research serves to perpetuate unfounded fears about potential pandemics.
Question 24: How do the authors explain the role of nutrition in disease prevention and treatment?
The authors emphasize the crucial role of nutrition in disease prevention and treatment, contrasting it with the germ theory approach. They argue that many historical diseases attributed to pathogens, such as scurvy and pellagra, were actually the result of nutritional deficiencies. The authors suggest that proper nutrition is key to maintaining a healthy immune system and overall well-being. They criticize the medical establishment for often overlooking nutritional factors in favor of pharmaceutical interventions.
Measles Virus and Lanka:
The book discusses German biologist Stefan Lanka's challenge to prove the existence of the measles virus. Lanka offered a reward for scientific proof of the measles virus's existence and size. When a doctor claimed the prize by submitting six publications, Lanka refused to pay, leading to a legal battle. The authors describe how the case went through multiple courts, ultimately resulting in a ruling in Lanka's favor.
The book uses this case to argue that there is no scientific evidence for the existence of the measles virus. The authors claim that the court case exposed the circular reasoning and lack of proper controls in virology. They suggest that this legal challenge undermines not just the concept of measles as a viral disease, but the entire field of virology.
Question 25: What criticisms do the authors present regarding the use of antibodies as proof of viral infection?
The authors strongly criticize the use of antibody tests as proof of viral infection. They argue that the presence of antibodies does not necessarily indicate the presence of a specific virus, as claimed by mainstream virology. The authors contend that antibody reactions can occur for various reasons unrelated to viral infections. They suggest that the interpretation of antibody tests is based on circular reasoning, where the presence of antibodies is used to prove the existence of a virus that was never properly isolated in the first place.
Question 26: How do the authors describe the historical development of vaccination programs?
The authors portray the historical development of vaccination programs as based on flawed science and driven by industry interests rather than public health concerns. They argue that the decline in mortality rates for many diseases occurred before the introduction of vaccines, primarily due to improved living conditions and nutrition. The authors claim that the expansion of childhood vaccination schedules since the 1980s has coincided with increases in chronic health issues. They suggest that vaccination programs have been promoted through fear campaigns and misleading statistics about their effectiveness.
Question 27: What is the authors' perspective on the concept of 'viral mutation' and its implications for vaccine efficacy?
The authors view the concept of 'viral mutation' as another unproven claim used to justify ongoing vaccination programs and research funding. They argue that since the existence of pathogenic viruses has not been scientifically established, the idea of viral mutations is baseless. The authors suggest that claims about mutations are used to explain vaccine failures and promote the need for regular booster shots. They contend that this concept serves to maintain public fear and dependence on the medical establishment.
Whooping Cough:
The book critiques the conventional understanding of whooping cough (pertussis) as a bacterial disease caused by Bordetella pertussis. The authors argue that the bacteria has never been proven to cause the symptoms associated with whooping cough. They discuss a 2006 incident at Dartmouth-Hitchcock Medical Center where PCR tests led to a false pertussis outbreak, using this as an example of how diagnostic tests can create the appearance of disease outbreaks.
The authors challenge the efficacy of pertussis vaccines, arguing that the historical decline in whooping cough mortality occurred before widespread vaccination. They suggest that factors like improved nutrition and sanitation are more likely responsible for the reduced impact of the disease. The book uses whooping cough as an example of how germ theory and vaccination programs persist despite what the authors see as a lack of scientific evidence.
Question 28: How do the authors explain the role of the immune system in health and disease?
The authors present a view of the immune system that differs significantly from mainstream medical understanding. They argue against the idea that the immune system needs to be "trained" or stimulated by vaccines to fight off pathogens. Instead, they suggest that a properly functioning immune system, supported by good nutrition and a healthy environment, is capable of maintaining health without artificial interventions. The authors contend that many symptoms attributed to infections are actually the result of the body's natural healing processes.
Question 29: What criticisms do the authors present regarding the use of RT-PCR tests for disease diagnosis?
The authors strongly criticize the use of RT-PCR tests for disease diagnosis, particularly in the context of COVID-19. They argue that PCR is a manufacturing technique, not a diagnostic tool, and that it cannot determine the presence of infectious particles or illness. The authors claim that the high sensitivity of PCR leads to the detection of irrelevant genetic fragments, resulting in false positives. They suggest that the widespread use of PCR testing has been the primary driver of the appearance of a pandemic, rather than reflecting a real increase in disease.
Question 30: How do the authors describe the process of pandemic declaration by health authorities?
The authors portray the process of pandemic declaration by health authorities, particularly the WHO, as arbitrary and driven by political and economic interests rather than scientific evidence. They argue that the criteria for declaring pandemics have been loosened over time to allow for more frequent declarations. The authors suggest that these declarations trigger pre-planned responses from governments and institutions, regardless of the actual health situation on the ground. They contend that this process serves to create the appearance of a crisis, justifying interventions that benefit the pharmaceutical industry and expand government control.
Question 31: What is the authors' perspective on the concept of 'vaccine hesitancy'?
The authors view 'vaccine hesitancy' as a legitimate response to flawed science and questionable practices in the vaccine industry. They argue that the term is used to stigmatize and marginalize those who question vaccine safety and efficacy. The authors suggest that increasing vaccine hesitancy is actually a result of more people becoming aware of the lack of scientific evidence supporting vaccination programs. They criticize efforts by health authorities and media to combat vaccine hesitancy, viewing these as attempts to suppress valid concerns and maintain the vaccine paradigm.
Question 32: How do the authors explain the role of fear in shaping public health policy?
The authors argue that fear plays a central role in shaping public health policy, particularly in relation to alleged pandemics. They contend that health authorities, media, and the pharmaceutical industry deliberately use fear-inducing narratives to promote compliance with interventions like vaccines and lockdowns. The authors describe how dramatic individual cases and misleading statistics are used to create a sense of widespread danger. They suggest that this fear-based approach prevents rational assessment of actual health risks and benefits of proposed interventions.
Question 33: What criticisms do the authors present regarding the concept of 'asymptomatic carriers' of disease?
The authors criticize the concept of 'asymptomatic carriers' as an unscientific idea used to expand the reach of medical interventions. They argue that this concept contradicts traditional understandings of disease and has been used to justify testing and restrictions on healthy individuals. The authors suggest that the idea of asymptomatic carriers is particularly problematic in the context of COVID-19, where it has been used to maintain the appearance of a pandemic despite many people testing positive without any symptoms.
Question 34: How do the authors describe the historical development of public health institutions?
The authors portray the historical development of public health institutions as a process increasingly influenced by pharmaceutical interests and flawed scientific paradigms. They argue that organizations like the CDC and WHO have shifted from addressing genuine public health concerns (such as sanitation and nutrition) to promoting drug and vaccine-based interventions. The authors suggest that these institutions have become mechanisms for implementing top-down health policies that often serve industry interests rather than public well-being.
Question 35: What is the authors' perspective on the future of medical science and public health policy?
The authors express hope for a future where the current paradigms of germ theory and virus-based disease models are abandoned. They envision a shift towards approaches that focus on environmental factors, nutrition, and supporting the body's natural healing processes. The authors argue for a complete reevaluation of current medical practices, particularly vaccination programs. They suggest that as more people become aware of the flaws in current medical science, there will be increasing resistance to centralized health policies and a move towards more individualized, holistic approaches to health.
I appreciate you being here.
If you've found the content interesting, useful and maybe even helpful, please consider supporting it through a small paid subscription. While everything here is free, your paid subscription is important as it helps in covering some of the operational costs and supports the continuation of this independent research and journalism work. It also helps keep it free for those that cannot afford to pay.
Please make full use of the Free Libraries.
Unbekoming Interview Library: Great interviews across a spectrum of important topics.
Unbekoming Book Summary Library: Concise summaries of important books.
Stories
I'm always in search of good stories, people with valuable expertise and helpful books. Please don't hesitate to get in touch at unbekoming@outlook.com
For COVID vaccine injury
Consider the FLCCC Post-Vaccine Treatment as a resource.
Baseline Human Health
Watch and share this profound 21-minute video to understand and appreciate what health looks like without vaccination.
Right or wrong I never lived a life in fear, That's why covid didn't affect nor infect me in the slightest. I just shook my head at the ridiculousness of what they were saying. Rabies, specifically, I investigated hard. That vaccine killed my dog and no one could tell me different.
The whole crux of covid was PCR. A simple google search laid that piece of bullshit to rest. Yet somehow no one seemed to care enough to investigate. They used a bogus test to claim infection and yet no one questioned the death of it's inventor 2 months before this planned experiment was formulated. I just don't know what to say in the face of that utter lack of common sense.
Peeling an onion can be hard