Besides the fact that Gardasil injured our son, I’m particularly interested in the HPV story because it’s the holy grail of the vaccine industry. It was the first bridge that connected the cancer complex with the virus, and its vaccine complex.
A cancer, with a virus to blame and a vaccine to fix it. It really doesn’t get more perfect than that. And all with an Australian origin story. I am particularly interested in the architecture of incentives and malfeasance, and this story has it all.
It’s quite an amazing read and a great insight into the vaccine industry generally and its ability to capture all and sundry.
I first understood the connection between the cancer complex and the virus complex (or as Duesberg would call them The Virus Hunters) when I read his amazing book Inventing the AIDS virus. I cannot recommend that book highly enough.
Not only is it a wonderful follow up to The Real Anthony Fauci (that first introduced me to Duesberg) but it’s the most important book to truly understand the rot in the AIDS industrial complex that Fauci built. I’ve said it before, the GMC we had to have is AIDS 2.0.
One of the main points Duesberg taught me was how the virus hunters invented “latency period” to explain why they weren’t seeing cancers in people that had the virus. I wrote about this in my first stack on the HPV vaccine.
Indeed, the evidence for the papilloma hypothesis has since fallen apart. When zur Hausen and his colleagues discovered that at least half the American adult population and, therefore, half the adult women, had been infected by the virus, yet only 1 percent of women develop the cancer in their lifetime, they began to see a discrepancy. Koch's first postulate has also tested the credulity of the cancer virologists, since at least one-third of all women with cervical cancer have never been infected by the virus. The rest of the cervical cancer patients are not all infected with the same strain of papilloma virus; over a dozen different varieties of the virus can be found in these women.
An incredibly long time elapses between infection by the virus (in those who do get infected) and the onset of the tumor. Papilloma virus tends to be contracted by women who are younger and more sexually active, estimated at an average twenty years of age. Cervical cancer, a disease of older age, strikes women in their forties through their seventies. By subtraction, zur Hausen calculates a whopping "latent period" ranging between twenty and fifty years! Nor does the virus reactivate when the cancer appears; in keeping with the revised Lwoff hypothesis of viral latency and cancer, scientists simply assume the virus caused some sort of necessary but not sufficient mutation twenty to fifty years earlier and can therefore remain soundly asleep in the tumor tissue. But this explanation cannot account for several key facts. For one thing, the leftover pieces of the virus cause entirely different, and therefore irrelevant, mutations in the genetic code of each tumor. Also, each cervical cancer grows from one single cell, leading to the obvious question of why all the other millions of infected cervical cells never develop into tumors.
Back in the 90s they were talking about 20-50 year latency periods. Duesberg called bullshit on that back then, that’s why they never liked him.
Now back to The HPV Vaccine on Trial book. Chapter 18 outlines the Australian origin story that I’m particularly interested in.
Here is that chapter with notes and commentary.
AUSTRALIA: FIRST TO INJECT
Australia is at the center of the HPV vaccine universe, although most people in the US are completely unaware of it. Australia conducted clinical trials for both HPV vaccines and was one of the first countries to recommend it for girls in 2007. It recommended the vaccine for boys in 2013. Cervical cancer is rare in Australia, with mortality rates even lower than in the Unites States, at 1.8 deaths per 100,000 women.
Let’s just stop and think about this for a moment. Australia with basically the lowest rate of cervical cancer in the world decided to go HPV vaccine crazy.
1.8 deaths per 100,000 women per annum.
They are jabbing the girls (and boys) in their early teens, and the average age of diagnosis of cervical cancer in Australia is 50. So, let’s say a latency period of about 40 years.
As I always say any jab needs to pass the NSE 3-legged stool test of Necessity (first) then Safety, then Effectiveness.
So, the powers that be, have deemed it necessary to jab 100,000 teenage girls to protect 1.8 of them, 40 years later, from dying of cervical cancer. Does that make sense to you?
The only way that Necessity equation would work is if:
It was PROVEN that ALL cervical cancer is caused by the HPV virus. It’s not.
That there was no other way of dealing with the problem in 40 years, such as early detection and treatments. There are.
That there will not be any innovation over the next 40 years in terms of detection and treatment. There will.
That the vaccine was 100% proven to work. It’s not.
That it is 100% safe. It is not.
To reduce a 1.8 per 100,000 risk, 40 years out, you need 100% absolute surety on these questions to run around and jab 100,000 teenage girls.
That surety does not exist, quite the opposite. And therein lies the recklessness and malfeasance in this industrial scam.
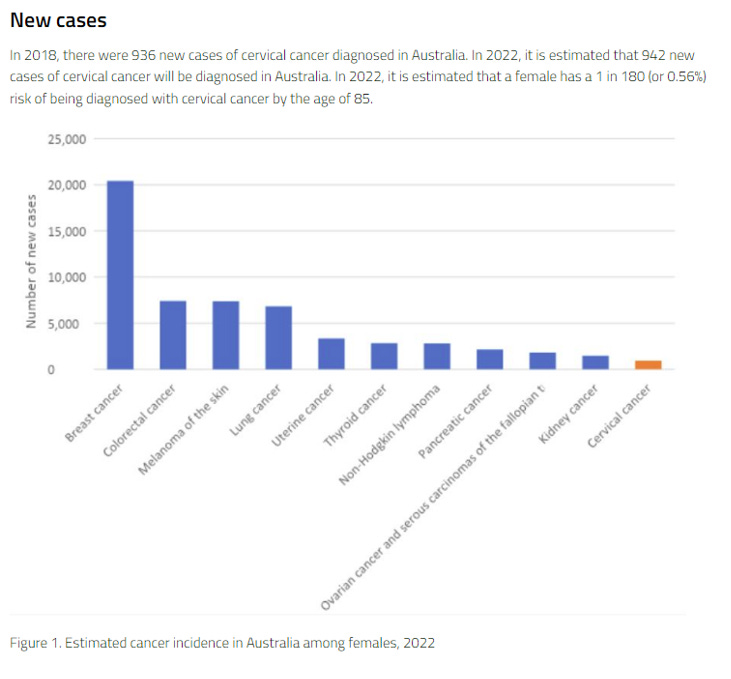
Also, while on the issue of necessity, here is a great chart about the number of new cases of cervical cancer in Australia relative to other cancers:
So, 942 estimated cases in 2022, of which 720 (76%) are estimated to survive.
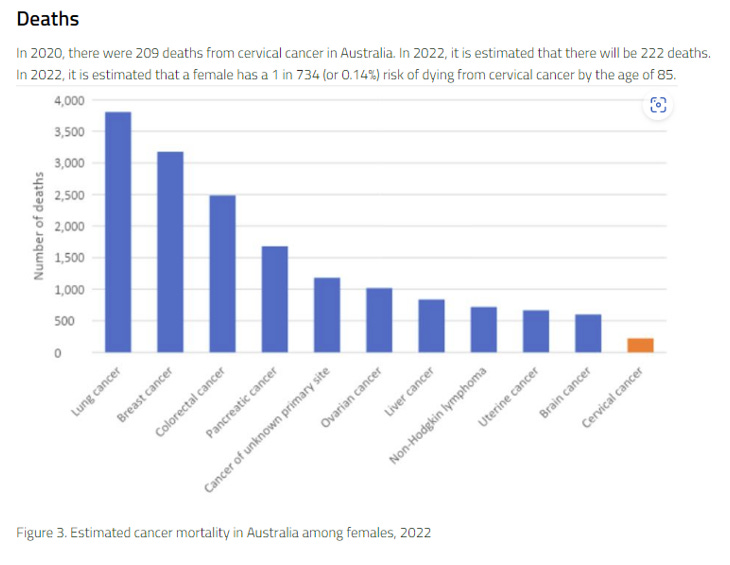
222 estimated deaths in 2022.
So, if 1.8 per 100,000 (or 222 in total) are too many requiring a national campaign to “treat” everyone, then what is the right number…is it Zero?
What would “success” look like in this realm…1.6 deaths per 100,000 or Zero deaths from cervical cancer?
It is the LEAST deadly cancer to women, yet 40 years ahead of time all teenage girls need to be “treated” with a cocktail that is KNOWN to be dangerous.
Does any of this make sense to you?
Also, how long do you think it will take for this industry to arrive at your daughter’s school with a “breast cancer vaccine” or a “uterine cancer vaccine”? Basically, every one of those cancers to the left of the cervical cancer bar will need to be “solved” and “eradicated” by coercion and force if necessary…for her own good.
Even before introducing the vaccine, Australia had the second-lowest cervical cancer rate in the world. But there are around 900 new cases annually, and tragically, around 250 women die of it each year.
Here is the current death chart, again relative to other cancers in Australia. It is the LEAST deadly female cancer.
Let’s now do a simple thought experiment, just for context and perspective.
Before the GMC (it’s higher now) we had about 160,000 deaths per annum split evening between men and women obviously.
So, about 80,000 Australian female deaths per annum, of which 222 will be cervical cancer.
Does this really look like the type of scourge to Australian women requiring a national, coercive campaign to inject all teenage girls?
Also, if your risk of dying from something is 1.8 per 100,000, that is a 1 in 55,555 chance of dying from it.
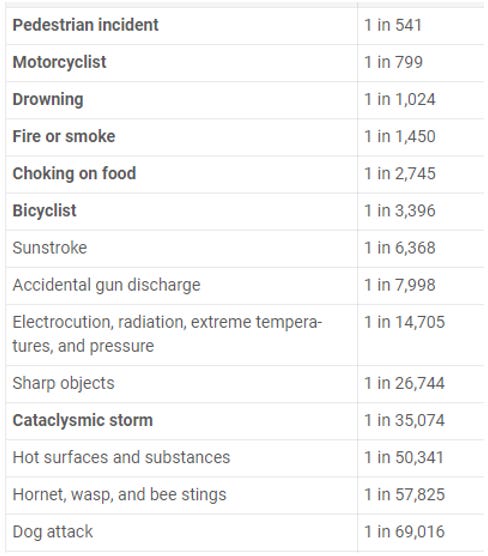
Let’s look at some other “chances of dying” numbers:
So, your risk of dying from cervical cancer (1 in 55,555) is on par with your risk of dying from a bee sting (1 in 57,825) and 50x LESS likely as your risk of dying from drowning (1 in 1,024).
If I came to you with a vaccine to protect you from dying from a bee sting, would you take it?
Should the government do a national, propagandised campaign to coerce you into getting it?
In indigenous communities where screening rates are low, cervical cancer rates are much higher. Only about 50 percent of indigenous women get regular Pap tests. As a result, they are four times more likely to die from the disease.
The HPV vaccine is an Australian invention, at least based on the 1990s patent wars. Professor Ian Frazer and Dr. Ian Zhou led the research team from University of Queensland that first produced an HPV VLP in a lab. Zhou died in 1999 before the world would see his invention. Professor Frazer continued their work, though, with the help of critical investment from Commonwealth Serum Laboratories (CSL), an Australian biotech company. Frazer and Zhou’s family own a general patent on VLP technology and also earn royalties on all HPV vaccines sold in the developed world. CSL has the exclusive rights to sell Gardasil in Australia and New Zealand, sharing profits with Merck.
Due to the international acclaim associated with the vaccine’s launch, Frazer became an Australian celebrity and the unofficial Australian spokesman for HPV vaccines. He is considered a “National Treasure” and received the “Australian of the Year” award in 2006, among other honors. One magazine even dubbed him “God’s gift to women,” for his contribution to women’s health.
As the FDA got closer to approving the vaccine in 2006 in the US, stakeholders in the Australian vaccine program assumed that regulators would approve adding the HPV vaccine to the national schedule without hesitation. In a surprising turn of events, however, Australia’s drug approval board, the Pharmaceutical Benefits Advisory Committee, rejected the Gardasil application in November 2006. The Advisory Committee based its decision on cost and efficacy. The then-Minister for Health, Tony Abbott, justified the decision by saying that the Committee had unanswered questions. According to an article in The Australian, he even floated the “bizarre idea that a misplaced confidence in the effectiveness of the vaccine might actually result in an increase in cancer rates.” He also said on a national radio show that he would not vaccinate his own daughters.
So, Tony Abbott, as Health Minister no less, said he wouldn’t give it to his three daughters.
The media reacted quickly to condemn Minister Abbott. Within 24 hours, Prime Minister Howard stepped up to allay public fears over what the Health Minister had said. The prime minister reassured the public that this “wonderful drug” that the public had been waiting for would be available without delay. In an unprecedented move, Prime Minister Howard stepped in to assure the Advisory Committee that the vaccine manufacturer would lower the cost if the Committee approved it. This assurance posed an ethical challenge to the Committee’s independence. Nonetheless, the Committee quickly reversed its previous decision and approved Gardasil. Prime Minister Howard then asked for the vaccine school program to begin in April 2007, six months ahead of schedule. CSL, which distributes the vaccine, agreed to accelerate the rollout. Australia would be the first country in the world to make it available as part of a national school immunization program, despite its low rate of cervical cancer.
I had no idea of any of this history. Clearly you only pay attention to that which directly affects you. It all went over my head in 2007. There are things about Howard that I’ve liked, but with the passage of time and a better understanding of the world he has diminished in my estimation. This is but another black mark on his record. His intervention for industry to get Australian teenagers injected with a dangerous chemical.
His apologists would say that he didn’t know, which may be true, that he was acting on “best advice” but how much of a useful idiot does one need to be before we stop forgiving them.
By the way, Howard oversaw the disarming of the Australian population, at the time I applauded him (as a sleepwalker), today I see it through an entirely different lens.
An armed population wouldn’t have this done to them. This is actually part of Howard’s legacy.
This decision was not without controversy. The prime minister’s unusual intervention in the Committee approval process led to an oversight review the next year. The Committee’s Health Policy Monitor Marion Haas noted that a perceived willingness to interfere in the recommendation process might incentivize manufacturers and lobbyists to attempt to influence future Committee decisions. This would result in a loss of public confidence in the Committee and would undermine its independence. In the case of Gardasil, however, Ms. Haas did not recommend any corrective action or policy changes, as the public largely supported the Committee’s decision.
The Committee immediately endorsed the HPV vaccine, stepping over the controversy. Australia’s swift action showed the world its confidence in what they believed to be a lifesaving tool to prevent cervical cancer, developed by an Australian team. National pride helped lift the vaccine to market after fifteen years of hard work, and Ian Frazer himself injected the first girl in Australia, outside of the clinical trials. The stage was now set for other countries to follow suit. Many Western countries adopted national HPV vaccine programs within a few years.
This domino effect seems to be very real. We saw the domino effect after Italy locked down. Here we see it after Australia “fell” to the HPV lobby, and then other politicians and health bureaucrats simply look to the first domino and the herd stampede to conform and “hide” in the crowd begins.
Australian schools introduced the vaccine in April 2007. With uptake rates currently over 70 percent, the program is seen as a success. Since 2013, boys have been getting the vaccine too, with a consistent uptake of around 70 percent, as well. In 2013, the New York Times ran the headline “HPV Vaccines Showing Successes in Australia,” detailing reductions in warts and some high-grade cervical abnormalities after only four years. The article heralded Australia as a shining example of HPV vaccine uptake in contrast to lower uptake in the US.
The tragedy of giving this poison to boys is its own story. But understanding this timeline is especially relevant for me and our son as he got injected in 2014.
He was 15 years old here.
This is the origin of our son’s terrible hay fever. He never had it before Gardasil.
Soon after the vaccine’s arrival at schools, however, reports of adverse reactions began to surface. By May 2007, over AU$1 billion had been wiped from CSL’s share price in a jittery market reaction to the media reporting alleged adverse events. In one Melbourne school, 25 girls reportedly became sick, and five girls were hospitalized. By this time, the former Health Minister, Tony Abbott, who had famously criticized the vaccine’s introduction, was now prime minister. In a remarkable turnaround, he was now urging parents to continue to vaccinate their children, reassuring the public that the vaccine was safe.
This is the most galling part of the Australian story. Abbott’s unprincipled part. He intervened as Health Minister (who intervenes to stop a vaccine!?) knowing that it didn’t add up, clearly, he understood that at least one of the legs of the NSE 3-legged stool didn’t survive scrutiny.
But as Prime Minister, and under the pressure of the lobby and 2007 being an election year (in November) he decided they were safe and effective.
Conservatives are meant “conserve” that which is “right”, even if the mob wants to “progress”, but Australian conservatives stopped being that a very long time ago.
Shame on you Abbott.
Physicians treating the children echoed the prime minister, saying that the children’s health problems were not related to the vaccine. A CSL spokesperson announced that the girls had suffered a collective anxiety attack, not physical reactions. Ian Frazer too was quick to dismiss the girls’ reactions as psychosomatic and urged the public to appreciate the “cancer-preventing vaccine.” The share price recovered.
This “anxiety” trick is standard operating procedure in the HPV vaccine story. Because its given to teenage girls, it is assumed that all their complaints are “in their head”, they are teenage girls after all.
CSL has played an important role in introducing HPV vaccines in Australia. It is one of the country’s top twenty companies, now worth almost AU $50 billion (around US $40 billion). It earned AU$183 million (around US $140 million) from royalties and licensing fees in 2016–17, largely from Gardasil sales worldwide. The company earns 7 percent in royalties from Merck and 2 percent in royalties from GSK for licensing their HPV vaccine technology to the pharmaceutical giants. In a strange twist of fate, some girls who report autoimmune disorders following the HPV vaccine are recommended by their doctors to receive CSL’s IVIG (intravenous immunoglobulin) to treat their symptoms. IVIG products are a “key growth driver” at CSL. Who’s to say if this is a coincidence?
Immunoglobulins (Ig) represent our largest therapy area and contributed sales of US$2,774 million, up 14% in constant currency over last year. Intravenous immunoglobulin (IVIG) sales growth was underpinned by solid global demand for PRIVIGEN®, Immune Globulin Intravenous (Human) 10% Liquid, with sales up 21% in constant currency over the prior comparable period. Excellence in execution, a focused approach to growth in the non-acute segment, and use of PRIVIGEN to treat chronic inflammatory demyelinating polyneuropathy (CIDP) contributed to this impressive growth.
Sales of our subcutaneous immunoglobulin product, HIZENTRA®, Immune Globulin Subcutaneous (Human) 20% liquid, increased by 10% at constant currency, led by strong demand in the US and Europe. New patient starts on HIZENTRA and patients converting from IVIG were key drivers of growth, particularly in Belgium, France, United Kingdom, the Nordic region, Brazil and Mexico.
CIDP is associated with vaccine injury.
What they have done, is basically rebrand GBS (Guillain Barre Syndrome) that is widely accepted as an auto-immune vaccine injury.
CIDP is chronic GBS, so it’s a wonderful relabeling to hide GBS.
So CSL is profiting at both ends of the game and crowing about its “impressive growth” in the GBS market.
A neurological disorder, CIDP disease causes weakness and decreased sensations in your limbs.
Guillain-Barré Syndrome (GBS) is a disorder where your body's immune system attacks your peripheral nerves. Chronic inflammatory demyelinating polyneuropathy (CIDP) is the chronic form of GBS.
To understand typical CIDP, you need to first learn about your Myelin sheath’s role in your body. Myelin is an insulating layer of proteins and fat. This layer forms around your nerve fibers, including the ones in your spinal cord and brain. Myelin protects your nerves and their ability to transmit body signals quickly.
When something damages your myelin, your nerves lose their protection. This can damage your peripheral nervous system and disrupt the signals between your nerves and brain. Disruption of these signals leads to sensory loss, numbness, tingling, muscle weakness, or paralysis in the limbs, resulting in difficulty walking.
CIDP is an autoimmune disease that causes your body's immune system to attack your myelin sheath. A foreign infection can trigger this immune response. Unfortunately, the flu shot and other common vaccines in the United States act as foreign infections that can cause this rare disease, CIDP.
What’s interesting is that CSL does not mention Gardasil in its current annual reports. It’s as if they’d rather forget. That makes sense when you understand where the class action lawsuits are at in the US.
Australia is committed to reporting and studying the side effects to HPV vaccines through the Department of Health’s Therapeutic Goods Association (TGA) using its Database of Adverse Event Notifications, or DAEN, system. From April 2007, when the vaccine was first introduced in schools, to March 2018, there were around 4,300 reported adverse events, including one death.
What we now know is that severe under-reporting is the norm when it comes to vaccine injury.
41x under-reporting in the Covid jab space, across the board, is at the low end of the range for many injuries.
Just as in other countries with documented reports of serious adverse events after vaccination, the TGA denies any causal association. But like in the US, UK, and Ireland, the TGA receives critical funding from industry in licensing fees. This funding may create conflicts of interest, despite the promise of regulatory oversight.
In 2015, the TGA published Australia’s most recent in-depth report on adverse events following the vaccine for the year 2013. The adverse event rate in girls was 122 per 100,000 and 101 per 100,000 in boys 12-to-13-years old.
If we apply our 41x metric, the truer per 100,000 adverse event number would be 5,002 in girls (or 1 in 20) and 4,141 in boys (1 in 25).
A politician might not know this, but the medical establishment pushing these injections and manipulating the politicians does. Ian Frazer knows, or ought to know. He has no excuse for not knowing.
Interestingly, for boys aged 14 to 15, the rate decreased to 44 per 100,000 doses, with no reason given as to why. Is there a reason why younger boys have more than twice the reactions that older boys have? The reaction rate for girls is seventeen times the incidence rate for cervical cancer throughout the life span, but this is not examined.
This 17x difference is NOT true. It assumes no under-reporting.
It is based on about 7 CASES of cervical cancer per 100,000 women vs 122 adverse events per 100,000. But the truer number is 5,002 adverse events per 100,000.
So, 7 vs 5,002 is 714x, not 17x.
How’s that for a risk benefit calculation?
All adverse events were considered mild, and the report only looked for acute reactions in 2013 and did not consider long-term ones. The report also looked only at anaphylaxis, fainting, allergic reactions, and conditions that required hospitalization. The TGA did not review other conditions or clusters of symptoms in the 748 reports filed that year.
When the TGA published this information on its website, it prefaced the data by mentioning three other conditions of interest in 12- and 13-year-olds: demyelinating disorders, complex regional pain syndrome (CRPS), and premature ovarian failure (POF). The TGA stated that it looked at “a few” cases of demyelination disorders, such as multiple sclerosis, reported after Gardasil. However, it found “no evidence that the incidence of demyelination disorders after Gardasil vaccination is higher than would occur by chance.” There were three cases of CRPS following the vaccine, but CRPS was considered to be “a very rare adverse event associated with the injection rather than the vaccine itself.” Since CRPS is an autoimmune condition, its causal association with injection rather than the vaccine is incomplete at best. Finally, the TGA looked at three POF reports and stated that the “condition is known to occur naturally in this age group” and that there was no evidence to suggest that Gardasil is the cause.
This is a good moment to reflect on Toby Roger’s recent post about Pharma Junk Science:
Actual science begins with proper methods, e.g.: • appropriate study design, • registered clinical trials, • large sample sizes, • long observation periods, • randomized, • double-blinded, • rigorous statistics, conducted by people following Mertonian norms of: • communalism, • universalism, • disinterestedness, and • organized skepticism.
Then there is Pharma junk science that is characterized by: • financial conflicts of interest, • manipulated study design, • captured regulators, • deviations from protocol, • small sample sizes, • short observation periods, • bad record keeping, • data manipulation, • inappropriate statistical analysis, • drawing sweeping conclusion from weak data, • suppression or censorship of data that does not fit a predetermined narrative, • bullying, gaslighting, and blacklisting of scientists who ask hard questions.
Knowing the difference between actual science and Pharma junk science is a matter of life and death these days.
The FDA and CDC do NOT engage in actual science. Everything they do is Pharma junk science. Those who fail to understand this fundamental truth are not going to make it.
Said another way, there is Real Science (that which is honest and true) and there is Junk Science (that which isn’t) and Pharma are the global leaders of Junk, Industrialised, Junk Science.
When you read sentences like:
“The TGA did not review other conditions or clusters of symptoms in the 748 reports filed that year.”
THAT is Junk Science right there.
There may be no conclusive evidence that Gardasil is the cause, but the TGA statement that POF occurs naturally in this age group has no basis in fact. POF, meaning in essence permanent infertility in many cases, is a devastating diagnosis. To say that it is “known to occur naturally” at 13, which is the age group the TGA looked at, is simply a distortion of the truth. Dr. Deirdre Little, with over thirty years of clinical experience in New South Wales, published an article on POF cases she observed in her practice, which we discuss in Chapter 10. She wrote that the “age-specific incidence of idiopathic POF in early to mid-adolescence is so rare as to be unknown.” Despite Dr. Little’s best efforts to bring the TGA’s attention to these cases, the Australian government and scientific community have largely ignored her research.
Here is Dr. Little
AUSTRALIA’S HPV VACCINE CRITICS
Professor Ian Frazer denies that there are any long-term problems following HPV vaccination. Stephen Tunley, the Australian father of an injured daughter, disagrees. Stephen’s daughter received the vaccine in 2009; she became seriously ill after her second shot. He is dedicated to finding out how the vaccine may have caused the cascade of events leading to his daughter’s severe and chronic illness.
Steve’s research quickly took him to SaneVax, where he became acquainted with Norma Erickson and Freda Birrell. Steve agreed to join the SaneVax board in 2011 and has been an outspoken campaigner for HPV vaccine safety ever since. He has been featured in several media articles and has published comments in Lancet criticizing HPV studies.
Media heavyweights like the online research group The Conversation, to which Ian Frazer is a contributor, quickly attack any voices of dissent. Because of its support from thousands of universities and research institutes, The Conversation’s articles have been widely cited since 2010. Government agencies and industry also lend support to the vaccine, making dissent almost inaudible.
One critic who managed to get her voice heard was University of Wollongong PhD candidate Judy Wilyman. In 2015, she published a controversial doctoral thesis on Australia’s vaccination policies. Wilyman dissected the arguments for universal HPV vaccination and the assumptions underpinning the decision to adopt a national program. She highlighted the disparity between incidence and mortality in high versus low-resource countries, exposing the fallacy that HPV infection poses equal risk to all women. She criticized the Australian government’s involvement in marketing the HPV vaccine as cancer prevention when the clinical trials could not show this.
The University accepted her thesis and granted her a doctoral degree, but a media backlash ensued. A public petition with over 2,200 signatures demanded that the Australian Department of Health intervene and issue “unequivocal condemnation of this travesty,” amid accusations of “gross academic misconduct at the University of Wollongong.” The petition accused the University of supporting “dangerous myth-making.” An article in The Australian criticized her “antivaccine” stance and, by association, the University. Her doctoral supervisor, Professor Brian Martin, vigorously supported Dr. Wilyman’s research and intellectual freedom. Professor Martin published many retorts to accusations from The Australian and other blogs on his private website, defending her thesis and the University’s doctoral procedures.
GARDASIL 9 IN 2018
In late 2017, at a dramatic press conference on Australia’s Bondi Beach, Prime Minister Malcolm Turnbull announced that Gardasil 9 would replace Gardasil in schools beginning the following September. He proclaimed, with Ian Frazer by his side, that it was possible to completely eliminate HPV through vaccination.
“Eliminate” means Zero HPV.
Where have we heard “Zero” before?
Zero Covid.
Zero Carbon.
Zero anything does not map over reality and it’s both authoritarian and totalitarian in nature.
Anyone that mentions Zero anything, in any way, should be shunned and removed from positions of power and decision making.
As it turns out, our ex. Prime Minster Turnbull became a true Covid zealot, promoting the jab, promoting the “health care” response and is also promoting climate policies.
He has been doing his bit for the global cause for some time.
Mr. Turnbull seized the moment to promote the vaccine against the backdrop of the world-famous surfing beach, repeatedly referring to the vaccine as “lifesaving,” just like the lifeguards behind him. Adopting Gardasil 9 also coincides with a new two-dose schedule to bring Australia into line with other countries that had reduced the number of doses from three to two in 2015–16.
Australia has succeeded in maintaining relatively high HPV vaccination rates, at least in part because of an effective public relations apparatus. The vaccine is a source of pride for the Australian government, and it is using this invention to promote the country as a center for excellence in scientific research and development. With Professor Frazer leading the campaign toward universal Gardasil 9 uptake in 2018, the voices of the injured will likely remain all but unheard.
Thank you for reading this Substack.
Please share with others, we need to grow the resistance. Especially in Australia!
Please consider a small paid subscription (donation). The money goes to a good cause.
I am always looking for good, personal GMC and stories. Shared stories help others.
In the comments, please let me know what’s on your mind.
It makes zero sense, other than as a sterilization/ depopulation tool.
I have 4 daughters and never let any of them take it. If they did it later behind my back, I have no idea, but they all knew how I felt about it.
I am so sorry your son was injured and for all the young people that were injured whose parents haven't made the connection, as well as all those that will be injured by this criminal medical intervention!
I had no idea Guardasil was developed in Australia. I read about many girls in the Netherlands being paralyzed, severely injured or killed by them when researching it years ago.https://sanevax.org/hpv-vaccines-a-danish-documentary/
"..An armed population wouldn’t have this done to them. This is actually part of Howard’s legacy..."
How would the ownership of higher powered guns..reversed/stopped etc etc a govt mandated, industry supported,science supported piece of quackery like this vaccine?













It makes zero sense, other than as a sterilization/ depopulation tool.
I have 4 daughters and never let any of them take it. If they did it later behind my back, I have no idea, but they all knew how I felt about it.
I am so sorry your son was injured and for all the young people that were injured whose parents haven't made the connection, as well as all those that will be injured by this criminal medical intervention!
I had no idea Guardasil was developed in Australia. I read about many girls in the Netherlands being paralyzed, severely injured or killed by them when researching it years ago.https://sanevax.org/hpv-vaccines-a-danish-documentary/
"..An armed population wouldn’t have this done to them. This is actually part of Howard’s legacy..."
How would the ownership of higher powered guns..reversed/stopped etc etc a govt mandated, industry supported,science supported piece of quackery like this vaccine?