


The House That AIDS Built
By Liam Scheff


This short clip, of Stanley Plotkin being interrogated by Aaron Siri, reminded me of Liam Scheff.
I haven’t written about Liam in a while.
If you are new to this substack and haven’t read Official Stories, by Liam, I can only recommend that you do. It remains one of the most important books I have ever read.
Official Stories: Counter-Arguments for a Culture in Need: Scheff, Liam
It was Liam’s only non-fiction book, self-published because nobody else would touch it. Liam is no longer with us.
Some time ago, a reader, Tom Busse, posted this comment, in response to the Toby Rogers review of Official Stories.
It's worth noting Liam Scheff as a journalist broke one of the deepest, most disturbing, stories ever by any investigative journalist: https://altheal.org/toxicity/house.htm Also, I have his original art - he got into comic book art illustrating the official stories. I was glad to know him.
Tom is referring to one of the most important stories that Liam broke titled The House That AIDS Built.
I’ve been meaning to republish it to amplifying its reach for some time, but watching the squirming smug Plotkin bumped it up my list.
This is the “industrial complex”, it’s institutions and it’s chosen people that have produced The Spanish Flu, Polio, AIDS, Virology, Vaccination, COVID (AIDS 2.0), to name but a few of their creations.
This is a mature supra-national complex that is a most vital part of our Invisible Empire.
With thanks and gratitude to Liam Scheff. You are missed.
The House That AIDS Built
Liam Scheff
This article deals with pharmaceutical abuse in a children’s home in NYC. This piece was investigated and written in summer through winter of 2003 and published in January 2004, with occasional updates. The story broke wide in early 2004, with coverage in the New York Post and the New York Press. It served as the basis of investigation for the BBC film "Guinea Pig Kids," and has prompted further investigation by the Associated Press - as well as a pointed attack by the New York Times. The investigation is ongoing.
Liam Scheff. E-mail : liamscheff@yahoo.com
Introduction:
In New York’s Washington Heights is a 4-story brick building called Incarnation Children’s Center (ICC). This former convent houses a revolving stable of children who’ve been removed from their own homes by the Agency for Child Services. These children are black, Hispanic and poor. Many of their mothers had a history of drug abuse and have died. Once taken into ICC, the children become subjects of drug trials sponsored by NIAID (National Institute of Allergies and Infectious Disease, a division of the NIH), NICHD (the National Institute of Child Health and Human Development) in conjunction with some of the world’s largest pharmaceutical companies – GlaxoSmithKline, Pfizer, Genentech, Chiron/Biocine and others.
The drugs being given to the children are toxic – they’re known to cause genetic mutation, organ failure, bone marrow death, bodily deformations, brain damage and fatal skin disorders. If the children refuse the drugs, they’re held down and have them force fed. If the children continue to resist, they’re taken to Columbia Presbyterian hospital where a surgeon puts a plastic tube through their abdominal wall into their stomachs. From then on, the drugs are injected directly into their intestines.
In 2003, two children, ages 6 and 12, had debilitating strokes due to drug toxicities. The 6-year-old went blind. They both died shortly after. Another 14-year old died recently. An 8-year-old boy had two plastic surgeries to remove large, fatty, drug-induced lumps from his neck.
This isn’t science fiction. This is AIDS research. The children at ICC were born to mothers who tested HIV positive, or who themselves tested positive. However, neither parents nor children were told a crucial fact -- HIV tests are extremely inaccurate.(1,2) The HIV test cross-reacts with nearly seventy commonly-occurring conditions, giving false positive results. These conditions include common colds, herpes, hepatitis, tuberculosis, drug abuse, inoculations and most troublingly, current and prior pregnancy.(3,4,5) This is a double inaccuracy, because the factors that cause false positives in pregnant mothers can be passed to their children – who are given the same false diagnosis.
Most of us have never heard this before. It’s undoubtedly the biggest secret in medicine. However, it’s well known among HIV researchers that HIV tests are extremely inaccurate – but the researchers don’t tell the doctors, and they certainly don’t tell the children at ICC, who serve as test animals for the next generation of AIDS drugs. ICC is run by Columbia University’s Presbyterian Hospital in affiliation with Catholic Home Charities through the Archdiocese of New York.
Sean and Dana Newberg are two children from ICC. Their mother used drugs and was unable to care for them properly, so they were raised in foster care, until their great-aunt Mona adopted them. Mona Newberg is a teacher in the New York Public Schools, and has her Master’s degree in Education. She adopted the children when Sean was three and Dana was six. She was already raising their older brother, who was never given an HIV test or AIDS drugs. He’s now grown, healthy and serving in the Navy.
Their mother used heroin and crack cocaine since she was a teenager. She was given an HIV test in the late 80s and tested positive. “She had three children before Sean and Dana,” said Mona. “Nobody told us that the test cross-reacted with drug abuse, let alone pregnancy. It’s not a valid test.”
Because of the test result, the doctors at Columbia Presbyterian put Sean on AZT monotherapy when he was 5 months old. Use of AZT monotherapy is now considered malpractice because it can cause debilitating, fatal illness including fatal anemia.
Dana spent her first four years at Hale House, a NY orphanage for children whose parents abused drugs. Hale house was participating in an AZT drug trial when Dana was there. “We can’t get the records from Hale House, so I don’t know what happened there,” Mona said. “I never gave Dana the drugs after I got her, but I know she arrived with a filled prescription for AZT.”
Sean has been on life support twice as a result of the AIDS drug Nevirapine. Dana was put on AIDS drugs in 2002, even though she wasn’t sick. Since being put on the drugs, Dana has developed cancer.
Both children have been taken into ICC and kept there against their will and against Mona’s wishes for one reason – Mona has questioned the safety of the AIDS drugs AZT, Nevirapine and Kaletra and stopped giving the drugs when they made the children ill. In the summer and fall of 2003, I visited Mona, Sean, Dana and ICC. I spoke with Mona about her experience and her decision. (The names of Sean, Mona and Dana are aliases which they requested to protect their identities, but their stories are accurate and unaltered).
Liam Scheff: What led you to question the safety of the drugs?
Mona: When I first got Sean at three years old, he was a vegetable. He’d never eaten solid food. He had a feeding tube that went through his nose into his stomach. AIDS medications change the taste buds. AZT, especially, makes it so kids can’t stand the taste of food and won’t eat. The nurses fed Sean AZT, Bactrim and six cans of Pediasure a day through this tube, which stayed in his stomach for over two years. Nobody ever bothered to change it.
When I got Sean, I continued to give him the drugs as prescribed for about 5 months. But after each spoonful, he got weaker. I thought, wait a minute – this stuff is supposed to be making him better, why is he getting worse?
Sean had night sweats and fevers 24 hours a day. He had no energy. He couldn’t play. He couldn’t get up for ten minutes without lying down. Nurses came regularly to give him blood infusions to manage the AZT anemia. After the infusions, he’d be nearly comatose for two days. He was like a limp doll.
Every time I gave Sean the drugs, he got weaker and sicker. I didn’t know what to do but I didn’t want him to die. So I stopped everything that appeared to be killing him. I stopped the AZT. I stopped the Bactrim. I stopped the nurse from coming to give the infusions.
It wasn’t immediate, but Sean started to improve. His fevers subsided. He could eat. He gained weight. Within a couple months, he was actually running and playing with the other children. Sean was born with a chronic lung condition because of his mother’s drug use, but even his lungs improved. I couldn’t believe it. When Sean was born, the doctors told his mother that he was going to die. They told her to buy a coffin for him. He barely survived. When I took him off the drugs, he was healthy for the first time in his life.
I was so happy, I told everyone - including the doctors and nurses - what had happened. I didn’t know not to. When the hospital found out I wasn’t giving him the drugs, they contacted Agency for Child Services (ACS). An ACS worker came to my door, and told me I had to register the kids with an infectious disease doctor – Dr. Howard at Beth Israel. I was taking Sean and Dana to a Naturopathic MD, and they were both healthy and strong. I told them that we had a doctor. They said, “Too bad, you have to see Dr. Howard now.”
Howard was terrible for the children. He ignored the only thing that actually bothered Sean – his lung condition, and insisted that he go on a new drug for HIV. He said, “There’s a new miracle drug. It just came on the market. I guarantee if you give it to Sean, you’ll watch the miracle happen”.
LS: What was the miracle drug?
Mona: Nevirapine. Howard put Sean on Nevirapine. Sean’s health immediately deteriorated. He got sicker, his lungs congested, he lost weight, his cheekbones sunk, his liver and spleen started to go. Six months after he went on Nevirapine, he had complete organ failure. He was on life support for two weeks at Beth Israel Hospital. Then I did some research on Nevirapine, and found out that it caused organ failure and death. When Sean finally got out of the hospital, Howard discharged him on hospice care. Six months earlier, he was healthy. Now they were telling me to prepare for his death.
Once I got him home, I stopped giving Sean the Nevirapine, and he was able to eat again. He started to gain some weight back. Sean was so weak after being on life support, with all those tubes in him. He’d gotten so thin. But he finally started to recover. When I took Sean to Dr. Howard, he was always surprised to see that Sean was improving. Howard would ask me, “Are you sure you’re giving him the medication, Mrs. Newberg?”
LS: In times of improvement, he suspected that you weren’t giving Sean the Nevirapine?
Mona: Right. He only worried when Sean wasn’t sick! AIDS doctors always think there’s something wrong if you’re not dying.
After that Howard started keeping Sean in the hospital for longer periods of time for the lung problems we used to treat at home. Howard kept Sean for 25 days and fed Sean the Nevirapine himself. Sean ended up back in intensive care with organ failure. He was placed on life support for two weeks. He got a hospital staph infection because Howard wouldn’t let him leave. He was eight years old, and just wanted to come home.
A month later, the hospital finally discharged him. Then ACS called me for a meeting. The ACS worker told me I should put Sean into Incarnation Children’s Center until he was stronger. They told me that ICC was this wonderful place. They said in four months he’d be strong enough to come back home. ICC took Sean off the Nevirapine and put him on Viracept, Epivir, Zerit and Bactrim. Sean improved off the Nevirapine, but the new drugs definitely made him sick – just not as badly. He had trouble walking, and his arms and legs got even thinner.
I visited Sean at ICC for five months. Then, when I wanted to bring him home, they said, “We don’t recommend that Sean leave here. You have a reputation for not giving meds.”
LS: ICC refused to let Sean come home?
Mona: Right. They kept him for a year and a half. I had to get a lawyer to get him out.
LS: What was it like for Sean at ICC?
Mona: There were children in wheelchairs, on crutches, with deformations. There were AZT babies. Their heads have a different shape, with the eyes spaced wide and sunken in. The drugs cause severe developmental problems. Many children have misshapen, weak limbs and distended bellies. Many are learning disabled. The kids at ICC are constantly medicated with all kinds of drugs. When children refuse the drugs the nurses hold them down and force feed them. Sean wanted to get the hell out of there.
During my visits I noticed that many children at ICC were walking around with tubes hanging from their undershirts, and I wondered what they were. Then one day, I saw the nurse come in with a whole tray of medications and syringes, and I watched her inject this medication into the tubes coming out of their stomachs. I couldn’t believe it. I thought, my god, what’s going on here?
Every child who had a stomach tube took their medication that way, from the three-year-olds to the teenagers. It horrified me. I couldn’t understand it. When I found out what was being done, I thought, surely this must be illegal. There’s no way they could be doing this legally.
I expressed my concerns to Sean’s ACS case worker. I said, “Do you know what they’re doing to those kids in there? This reminds me of Nazi Germany.” He said, “They’re doing wonderful things for these children.” I called Albany, the state capital, and talked to Dan Tietz at the New York State Department of Health’s AIDS Institute. He said, “What are we going to do if these little children refuse to take the medication? How are we going to save their lives if we don’t perform this operation?”
LS: Who performs this operation?
Mona: The children are sent to Columbia-Presbyterian for the operation. The surgeons there do it.
I was at ICC one day, and saw a fourteen-year old boy named Daniel refusing the pills. I actually saw him run from the nurse when she came to give him his medication. He said, “The medication makes me sick and I don’t want to take it.” His aunt was there, and she said, “The medication makes him very ill.”
The ACS case worker, Wendy Wack, came in, and said to the aunt very clearly, “Daniel has refused to take his medication. We’ve changed it three times and he’s still refusing. Now, the only thing left is the operation.” She said, “If you refuse the operation, we’ll call Agency for Child Welfare – and take Daniel away from you.” His aunt signed, and they took Daniel away. When he came back a few weeks later, he had a tube in his stomach.
LS: Does Sean have the tube?
Mona: No. He doesn’t want that tube in his stomach. He’s been there long enough to know you get the tube if you say no to the medication. He’s terrified, so he never refuses the drugs.
The children at ICC who don’t have the tubes tend to be a whole lot healthier and live a whole lot longer than the ones with the tubes.
I was talking to a boy named Amir. He’s 6. His stomach was so swollen. He said, “My stomach is swollen, it got big.” He said, ”They cut me,” and he showed a little cut on his side. He’s had a tube for a long time. Amir was an AZT baby. His face has that wider shape. He also has lypodystrophy from the drugs. He has huge fat lumps on his back and neck. They’ve taken him away for surgery twice but the lumps grow back.
Sean’s little friend Jesus just died. He was 12. He had a tube. He had a stroke from the drugs. There was a little girl, Mia. She had a tube. She had a stroke and went blind. She died recently too. Carrie, a 14-year-old girl died last year. She had a tube. There’s a three-year-old, Patricia. She’s had a tube since she arrived. She’s going home with it in her. I don’t think she’s going to make it.
I used to talk with the child care workers about the drugs. I got to know all of them and they were all very friendly with me. I said, “These drugs are killing the children.” They said, “We know.”
LS: They agreed with you?
Mona: Yes, but what can they do, they just take care of the kids. The doctors and nurses give the medication. Telling the doctors that the drugs make you sick doesn’t do anything. They just stare at you blankly. They don’t care. Compliance is the main goal of ICC. All the kids in ICC come from families who’ve failed to comply with the drug regimen.
LS: ICC is part of a national program running AIDS drug trials. Have you ever signed a waiver permitting them to use your children in a drug trial?
Mona: No, never. But ACS has signed for me when I didn’t want to give Sean drugs. When I said, “No,” the ACS case worker grabbed the form and said, “I’ll sign it. You don’t need to.” They’re always switching medications – they never ask me if it’s okay.
Right now, most of the kids at ICC are on Kaletra. Kaletra was on fast-track approval. It was released before testing was complete. But they do know something about Kaletra. It causes cancer. It says on the label, that this drug causes cancer in test animals.
I fought for a year to get Sean home. ICC wanted to put him in a foster home where someone would be paid to feed him the drugs every day. I got a lawyer and we finally got Sean out of there. My lawyer was able to get Sean’s ICC medical records. He told me, “Sean was tortured at Incarnation. He was tortured.”
Photos from ICC

Drugs used in clinical trials conducted at ICC, Columbia Presbyterian
and at hundreds of participating hospitals in pediatric AIDS clinics nationwide:
Drug: Retrovir (AZT)
Drug Company: GlaxoSmithKline
Known Toxicities (manufacturer's label):
"Retrovir (AZT) has been associated with hematologic toxicity, including neutropenia and severe anemia."
"Prolonged use of Retrovir has been associated with symptomatic myopathy (muscle wasting)."
"Lactic acidosis and severe hepatomegaly with steatosis, including fatal cases, have been reported with the use of nucleoside analogues (Retrovir, Epivir, Zerit) alone or in combination."
"Retrovir is not a cure for HIV infection."
"The long-term effects of Retrovir are unknown at this time."
"The long-term consequences of in utero and infant exposure to Retrovir are unknown, including the possible risk of cancer."
Drug: Epivir (3TC, Lamivudine)
Drug Company: GlaxoSmithKline
Known Toxicities (manufacturer's label):
"Parents or guardians should be advised to monitor pediatric patients for signs and symptoms of pancreatitis."
"EPIVIR is not a cure for HIV infection."
"Patients should be advised that the long-term effects of EPIVIR are unknown at this time."
Drug: Zerit (Stavudine)
Drug Company: Bristol-Myers Squibb
Known Toxicities (manufacturer's label):
"Fatal lactic acidosis has been reported in pregnant women who received the combination of Didanosine and Stavudine with other antiretroviral agents."
"Zerit will not cure your HIV infection."
"There is limited information on the long-term use of Zerit."
Drug: Viramune (Nevirapine)
Drug Company: Boehringer-Ingelheim
Known Toxicities (manufacturer's label):
"Patients should be informed of: the possibility of severe liver disease or skin reactions associated with Viramune that may result in death."
"Severe, life-threatening and in some cases fatal hepatotoxicity, including hepatic necrosis and hepatic failure, has been reported in patients treated with Viramune."
"Severe, life-threatening skin reactions, including fatal cases, have included cases of Stevens-Johnson syndrome, toxic epidermal necrolysis."
"Viramune is not a cure for HIV-1 infection."
Drug: Ritonavir (Norvir)
Drug Company: Abbott Laboratories
Known Toxicities (manufacturer's label):
"Redistribution/accumulation of body fat including central obesity, dorsocervical fat enlargement (buffalo hump), peripheral wasting, breast enlargement."
"Lipid Disorders."
"Substantial increases in the concentration of total triglycerides and cholesterol."
"Norvir is not a cure for HIV infection."
Drug: Kaletra (Ritonavir + Lopinavir)
Drug Company: Abbott Laboratories
Known Toxicities (manufacturer's label):
"Long term carcinogenicity studies of Kaletra in animal systems have not been completed."
"In male mice, there is a dose-dependent increase in the incidence of both adenomas and carcinomas (malignant tumors) in the liver."
"Kaletra is not a cure for HIV infection."
"The long-term effects of Kaletra are not known at this time."

Photos of an infant with Stevens-Johnson Syndrome, a blistering, peeling, potentially fatal skin rash. It is one of the known side-effects of the AIDS drug Nevirapine. Nevirapine is one of the primary drugs being readied for distribution in Africa.
Eight of over 200 current or recent drug studies conducted at ICC
and Columbia Presbyterian (and 800 nationally):
http://www.icc-pedsaids.org/page4.htm www.clinicaltrials.gov
The Effect of Anti-HIV Treatment on Body Characteristics of HIV-Infected Children
Conditions: HIV Infections; HIV Wasting Syndrome; Lipodystrophy
Sponsors: NIAID and NICHDThe Effects of Anti-HIV Therapy on the Immune System of HIV-Positive Children
Sponsors: NIAID and NICHDComparison of Stavudine Used Alone or in Combination with Didanosine in HIV-Infected Children
Sponsor: NIAIDHIV Levels in Cerebrospinal Fluid and Brain Function in Patients Receiving Anti-HIV Drugs
Sponsors: NIAID, NINDS (Nat. Inst. Neurological Disorders and Strokes), NARC (Neurologic AIDS Reseach Consortium)A Study of Lopinavir/Ritonavir in Infants with HIV
Sponsors: NIAD, NICHDA Study to Compare Different Drugs Used to Prevent Serious Bacterial Infections in HIV-Positive Children
Sponsors: NIAID, Pfizer, GlaxoThe Safety and Effectiveness of Valacyclovir HCI in the Treatment of Herpes Simplex or Varicella/Zoster Infections in HIV-1 Infected Children
Sponsors: NIAID, GlaxoThe Safety and Effectiveness of Treating Advanced AIDS Patients between the Ages 4 and 22 with Seven Drugs, Some at Higher than Usual Doses
Sponsor: NIAID, NICHD
The Doctor at ICC
To confirm Mona’s story, I spoke with Dr. Katherine Painter, the medical director of ICC. I asked her about AIDS drugs, clinical trials and the stomach surgery for children who can’t or won’t take the drugs. Dr. Painter told me that the greatest challenge facing children at ICC isn’t illness, but compliance with their drug regimen. She also confirmed that there are “loads and loads of studies being done on children.”
Liam Scheff: What does ICC do?
Dr. Katherine Painter (Medical Director of Incarnation Children’s Center): ICC deals with children who are medically complex but not acutely sick, and whose medical care provides more challenges than most. We’re having an increase in referrals over the last years to deal with medication adherence. There are a fair number of children whose HIV illness may be well controlled but whose families are experiencing difficulty complying with the child’s medication regimen.
What we’re asking of our families and patients in terms of adherence is something beyond 100% - All of their medicines all the time, whether they have them on-hand or not, whether the medication makes them sick, or whether they’re sick with a concurrent illness.
ICC is affiliated with Columbia Presbyterian. We work as a magnet for about six New York hospitals – Columbia Presbyterian, Harlem Hospital, New York Hospital, St. Luke’s/Roosevelt, King’s County Brooklyn and SUNY. We get referrals from outpatient HIV clinics in the city, in the five boroughs and in Westchester along the island. Most clinics are set up in medical centers.
LS: Does ICC participate in clinical drugs trials?
Painter: Many of the clinics that refer to us are participating in clinical drug trials. Children participating in a drug trial undergo monitoring, testing, and supply of an experimental drug through their outpatient clinic and we maintain that treatment here.
LS: When I search the Government Clinical Trial database, I find loads and loads of studies being done on children.
Painter: There are loads and loads of studies being done on children.
LS: I know that the medications are hard to take and have side effects. How do you get a child to take the drugs?
Painter: One of the issues with children is that they can’t swallow large pills. Many of the meds are horse pill size and come in multiple pills. The alternative liquid or powder formulations are not very palatable. They have a significant, lingering, bitter taste. We mix them with chocolate syrup. Some children can take this, others can’t. For some cases, it’s better administered through a Gastric tube.
LS: Is that the nose or stomach tube?
Painter: That’s the stomach tube. The nose tube is a Naso-Gastric tube. It’s appropriate for short term interventions. It has to be changed weekly from one side of the nose to the other to minimize sinus infection. You have to listen each time you push the medication or supplementation through the tube to make sure that the air bubbles you’re hearing are in the stomach, and not in the lungs, because it can be displaced.
LS: What’s a Gastric tube?
Painter: A Gastric tube (G-tube) goes through a small opening into the stomach.
LS: How do you put in a G-tube?
Painter: A surgeon does that. It’s done in the operating room, under anesthesia. The surgeon passes an endoscopy tube [a fiber-optic camera down the throat] which allows him to see the inside of the stomach. Then from the outside, the surgeon places the tube surgically
LS: He cuts through the abdomen?
Painter: Well, right, yeah, you’re actually cutting through the skin, through the abdominal wall musculature, and then through the stomach. It creates a very small hole, about a quarter inch. It takes several weeks to heal well, so it’s a bit tender. A small tube is placed through the opening or stoma. From the outside you can connect a syringe or feeding tube. The opening can be closed when not in use [by a plastic seal], which extends less than half and inch from the stomach. Some types are called buttons.
On the inside of the stomach is a device that holds the tube in place called a balloon, which is filled with water to a size that can’t be pulled back through the stoma.
LS: When is this surgery deemed necessary or appropriate?
Painter: When other interventions to help a child take a medicine by mouth have failed.
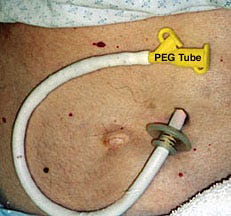

G-tube or PEG (Percutaneous Endoscopic Gastronomy) Tubes. G-tube Surgery.
The brochure for ICC reads – “a sanctuary of love, a home-like nurturing residence…”
Side Story:
Read The Nurse's Story: A pediatric nurse from ICC gives her account of successfully treating HIV positive children without AIDS Drugs.
Dana
In 2002, just as Mona got Sean back from ICC, the doctors decided that Dana (Sean’s sister) should be put on AIDS drugs, even though she wasn’t ill.
Mona: Dana wasn’t sick. She’d never had a major illness. The doctors said her Tcells were low, so he put her on Viracept, Epivir, Zerit, and Bactrim.
LS: What was her reaction to the drugs?
Mona: She was throwing up constantly. Over the next two months, she started complaining of back and head pain, which got so bad I had to take her to the emergency room.
Beth Israel diagnosed it as Langerhans Syndrome, which is a childhood disease similar to cancer. Langerhans affects bone. It damaged one of her vertebrae. It can be treated with chemotherapy, but it’s a low level dose, much lower than a standard cancer treatment.
Beth Israel knew about Dana’s HIV status. They told me, “We’re going to ship her over to Presbyterian for a new diagnosis. Because of her HIV status, there may be a possibility that this is AIDS.”
So they sent her to Presbyterian, where the doctor wrote in her records – “Langerhans Syndrome” but added, “May be associated with HIV.” Langerhans Syndrome is not an AIDS-defining illness. There is no entry anywhere in the medical record of an association between Langerhans and HIV. But Presbyterian called it AIDS and gave her a much stronger chemotherapy appropriate for an adult cancer. Then they switched her medication to Kaletra.
LS: Kaletra – that’s the fast-track approved drug that causes cancer?
Mona: Right. It states clearly in the manufacturers insert that Ritonavir – one of the ingredients in Kaletra – causes cancer in test animals, and that testing isn’t complete in humans. How do you give a child with cancer a drug that causes cancer?
The Kaletra made her heave and throw up. They were afraid that she’d become crippled if her back shifted in any way. So they put a brace on her to keep her still, and kept her on the drug. They gave her three months of chemotherapy, and the cancer was gone. They couldn’t find a trace of it. But they gave her another 3 months of chemotherapy anyway.
Right after her diagnosis in January (2003), Presbyterian called ACS and said I was putting Dana in jeopardy by not giving her the drugs. ACS took Dana out of our home and put her into ICC.
We went to court to get her back. Dana’s doctor at Presbyterian had to testify. When she was questioned under oath, she listed all the deadly side effects of the drugs - all of them. She knew exactly what all of them did. The judge asked her how she got the kids to take the drugs. And she said “We’re like Nazis when it comes to compliance.” Those were her words.
The Department of Health came to ICC three weeks ago for an inspection. They said that the children could no longer be restrained when they didn’t want to take the drugs. They said that the children didn’t have to take the drugs if they didn’t want to; they have a legal right to refuse medications. But the social workers and doctors told the children, “Sure you can refuse, but if you do there will be consequences.”
LS: What are the consequences?
Mona: The surgery.
Today Dana remains at ICC. She is 16. ACS is trying to put her in a foster home where she’ll live with a stranger who’s paid to give her the drugs. Mona is trying to bring her home. In August 2003, The Make-a-Wish foundation gave Dana the gift of a Disney Cruise to Bermuda. ACS told Dana that she was not allowed to leave the country, and cancelled her trip.
Sean’s blood is tested regularly to make sure that he’s taking the drugs. He’s been on AIDS drugs all his life. He weighs 51 pounds and is about 4 feet tall. Sean is now 13 years old.
During our interview, Dr. Painter of Incarnation Children’s Center told me that there was some good news about HIV. She said, “HIV is no longer a death sentence, it’s a chronic, manageable condition,” – as long as you take the drugs. But Jacklyn Herger (see link below to – “The Nurse’s Story” – part of complete story) and Mona Newberg both successfully treated pediatric AIDS without AIDS drugs. In fact, their children were most sick when the drugs were used. Is their experience valid? Is it reproducible? According to Incarnation Children’s Center, the answer is “Yes.”
From ICC’s published history: “Early in the [AIDS] epidemic, HIV disease of childhood was considered to be a downhill course leading to death. But in the late 1980’s, before AZT was available, many very ill children admitted to ICC got dramatically better with proper nurturing and high quality medical and nursing care.”
ICC successfully treated pediatric AIDS without toxic AIDS drugs. This startling revelation brings to mind a number of questions: Are the drugs necessary? Why are we using them if there are better options? And…
What Do We Really Know About HIV?
In July 2003, the esteemed science journal Nature Medicine published an article called “HIV-1 Pathogenesis” by AIDS researcher Mario Stevenson of the University of Massachusetts Medical School. The article was part of its “20 years of AIDS science” special edition.(6)
From the introduction:
"Despite considerable advances in HIV science in the past 20 years, the reason why HIV-1 infection is pathogenic is still debated... considerable efforts have gone into identifying the mechanisms by which HIV-1 causes disease, and two major hypotheses have been forwarded."
According to Stevenson, twenty years and 118 billion dollars in AIDS research (“considerable efforts”), have given no reliable proof as to how HIV might cause disease (“the mechanisms” by which HIV is presumed to be “pathogenic”). While it is always claimed that HIV is proven to cause illness, Stevenson spends the bulk of his review article pouring over what he describes as two “major hypotheses”that try to describe how HIV might work.
In science, a “hypothesis” is an idea or proposal about how something might work. A hypothesis isn’t a fact, it’s a guess that a scientist tries to prove is accurate and true. If a hypothesis fails, it’s discarded, so that new, better, more accurate ideas can be heard.
In the article Stevenson explains that we don’t know how HIV might damage, let alone kill cells, “…it is debatable whether lymphocyte [white blood cell] damage is due to the direct killing of infected cells...” and we don’t have any idea how HIV affects immunity, “…processes contributing to the immune activation state in HIV-1 infection are not well understood..." The HIV hypothesis states absolutely that HIV kills T-Cells, but Stevenson tells us the underpinning of this assertion is still debated.
Stevenson concludes the paper by returning to the main theme – the vast unknowns in HIV science:
"There is a general misconception that more is known about HIV-1 than about any other virus and that all of the important issues regarding HIV-1 biology and pathogenesis have been resolved. On the contrary, what we know represents only a thin veneer on the surface of what needs to be known."
Stevenson tells us that after 20 years of research into the various HIV hypotheses, we know "a thin veneer," about HIV's "biology and pathogenesis," that is, what HIV might look like, how it might work, and, as such, how - and therefore if - it is responsible for AIDS illnesses. We’re told that it is, but according to Stevenson and “Nature Medicine,”, we don’t have proof
By the standard of “First do no harm”if we don’t know how a molecule works (HIV or any other), then it is unethical to treat any presumed HIV positive person with extraordinarily toxic, and often fatal pharmaceuticals, which the manufacturers themselves admit, do not cure AIDS.
In addition to their long list of serious and potentially fatal side-effects, all major AIDS drugs also bear a version of this printed warning:
“This drug will not cure your HIV infection…Patients receiving antiretroviral therapy may continue to experience opportunistic infections and other complications of HIV disease…Patients should be advised that the long-term effects are unknown at this time.”
What Do HIV Tests Measure?
When you take an HIV test, your blood isn’t tested for a virus, it’s tested for your body’s natural antibody response to the proteins in the HIV test. These proteins are supposed to stand in for HIV.
In order for an antibody test to be clinically meaningful its proteins should accurately represent the proteins of a specific virus or particle.
But the proteins in the HIV test are not derived from purified viral particles, but rather from a variety of leukemia T-Cell cultures, or from synthetic production. A 1993 Bio/Technology paper gives an analysis of the nature of the HIV test proteins, and concludes that the proteins derived from these sources for HIV tests are, in fact, commonly-occurring (16).
http://www.virusmyth.net/aids/data/epwbtest.htm
The lack of specificity in the test proteins would seem to logically translate into a lack of specificity in the reaction to the test, but this is rarely addressed in the public conversation about HIV. However, the medical literature on HIV tests does call into sharp question their accuracy and utility. A comprehensive, updated list of citations on the tests can be found at the Albert Reappraising AIDS site: http://www.aras.ab.ca/test.html
All medical research can be challenged and disputed. But there is considerable evidence that the putative HIV test proteins occur commonly in both sick and healthy people. Unfortunately, the scientific community has tended to punish dissent and debate about popular and profitable paradigms like cancer and AIDS research. (For a good introduction to the problem of rigidity in flawed but profitable science, take a look at “The Cancer Industry” by Dr. Ralph Moss - http://www.ralphmoss.com/html/books.shtml
What does HIV-Positive mean?
The HIV test measures antibody response to these proteins. We produce “antibodies” to all the foreign material we encounter - germs, yeast, fungi, bacteria, pollutants, even food. Antibodies are proteins that are produced by our white blood cells to help identify foreign matter in our blood. They “grab” onto the foreign protein so that it can be processed safely.
Antibodies tend to be cross-reactive. That is, one antibody can grab onto a wide variety of proteins. The proteins in the HIV-test are commonly-occurring, and have demonstrated cross-reactions with a wide variety of antibodies. Given the non-specificity of the test proteins, and the variety of reactions to them, it would follow logically that the reaction of HIV tests should also be considered non-specific. It is, however, used as an entirely specific diagnostic tool.
How cross-reactive is the HIV-Test?
According to the medical literature, HIV tests can cross-react with antibodies produced from nearly 70 disease (and non-disease) conditions. These include yeast infections, arthritis, hepatitis, herpes, parasitic infections, drug use, tuberculosis, inoculations, colds and prior pregnancy (1-3). The HIV test is also more reactive with people who are chronically exposed to environmental stressors, bacteria, fungi, parasites and toxins (for example, people living in poverty without sufficient food and clean water, such as in Africa).
If you’ve been exposed to any of these conditions, it is possible that your body will produce antibodies that can react with the HIV test proteins.
Based on the extensive review of HIV tests in the medical literature, the term “HIV-positive” could be seen to have one non-debatable meaning: “Non-specific antibody to commonly-occurring protein-positive.” An HIV-positive test result may help identify patients who have a lot of antibodies in their blood. This might indicate a high historical exposure to illness, which might serve as a warning to better support immune function by improving general health. But a positive HIV test result on its own does not seem to be capable of indicating the absolute diagnosis a terminal, fatal virus or condition.
This is, of course, very different from what we’ve been told about HIV tests for 20 years. But the FDA and the test-makers are legally obligated to state the limitations of their tests. (From HIV test package inserts):
“At present there is no recognized standard for establishing the presence or absence of HIV-1 antibody in human blood.” (Abbott Laboratories HIV Test - ElA)
“The risk of an asymptomatic person with a repeatedly reactive serum developing AIDS or an AIDS-related condition is not known.” (Genetic Systems HIV Test - Peptide EIA)
“The AMPLICOR HIV-1 MONITOR test is not intended to be used as a screening test for HIV or as a diagnostic test to confirm the presence of HIV infection” (Roche, Amplicor HIV Test – PCR).
“Do not use this kit as the sole basis of diagnosis of HIV-1 infection.” (Epitope, Inc. HIV Test - Western Blot)
“[Positive test results can occur due to] prior pregnancy, blood transfusions... and other potential nonspecific reactions.” [Vironostika HIV Test, 2003].
The medical literature is also clear about the lack of specificity of HIV tests:
“False-positive ELISA [antibody] test results can be caused by alloantibodies resulting from transfusions, transplantation, or pregnancy, autoimmune disorders, malignancies, alcoholic liver disease, or for reasons that are unclear... The WB [Western Blot antibody test] is not used as a screening tool because... it yields an unacceptably high percentage of indeterminate results. ”
Doran TI, Parra E. False-Positive and Indeterminate Human Immunodeficiency Virus Test Results in Pregnant Women. Archives of Family Medicine. 2000 Sep/Oct;9:924-9.“False-positive HIV ELISAs have been observed with serum from patients with a variety of medical conditions unrelated to HIV infection.... False-positive HIV ELISAs [also] occur because of human or technical errors associated with doing the tests or because of antibodies that coincidentally cross-react with HIV or nonviral components in the tests... Notable causes of false-positive reactions have been anti-HLA-DR antibodies that sometimes occur in multiparous [pregnant more than once] women and in multiply transfused patients. Likewise, antibodies to proteins of other viruses have been reported to cross-react with HIV determinants. False-positive HIV ELISAs also have been observed recently in persons who received vaccines for influenza and hepatitis B virus”
Proffitt MR, Yen-Lieberman B. Laboratory diagnosis of human immunodeficiency virus infection. Inf Dis Clin North Am. 1993;7:203-19.
Regardless of what the FDA-mandated warnings or the clinical research tells us, these tests are used to tell people that they’re infected with a deadly virus.
The test makers are aware that HIV-positive test results occur because of “prior pregnancy, blood transfusion…and other nonspecific reactions,” “vaccines,” “human or technical errors,” “transfusions, transplantation, or pregnancy, autoimmune disorders, malignancies, alcoholic liver disease, or for reasons that are unclear.” Given all of this cross-reactivity…
How do we know who is really HIV-positive?
The answer to this question has more to do with sociology than science. Lab technicians, doctors and nurses are instructed by the test manufacturers to make this determination subjectively, based on socio-economic and sexual criteria.
The HIV test has two different names for similar or identical reactions: “nonspecific” and “specific.” A “nonspecific reaction” (HIV-negative or indeterminate) is the diagnosis given to people determined to be in the “low-risk group.” A “specific reaction” (HIV-positive) is the diagnosis determined to be in the “high-risk group.”
Social, Sexual and Economic Bias in HIV Testing:
Who are the people in these groups? The “high-risk group,” according to the test manufacturers, consists of “prison inmates, STD clinic patients, inner city hospital emergency room patients… homosexual men [and] intravenous drug users.” The “low-risk group” isn’t defined, but can be assumed to include people outside of poverty situations who are under less social, ethnic and economic stress.
For people in the “high-risk group,” an antibody reaction is more likely to be considered “specific” (HIV positive). However, for the “low-risk group,” the test manufactures state that “nonspecific reactions [HIV negative] may be more common than specific reactions [HIV positive]. (Vironostika HIV Test, 2003).”
What makes a “nonspecific” (HIV negative) reaction “more common” [more likely] than a “specific” (HIV positive) reaction in the “low-risk group”?
What makes a “specific” reaction “more common” in the “high-risk group?”
The answer to this question is different from test to test, lab to lab, and country to country. There are no standards for what makes a test “HIV-positive.”
“At present there is no recognized standard for establishing the presence or absence of HIV-1 antibody in human blood.” (Abbott Laboratories HIV Test - ElA)
The final analysis belongs to the subjective interpretation of the person or institution giving the test. The test manufacturers are telling the lab technicians, doctors and nurses who are reading these tests that it’s acceptable to determine HIV test results based on subjective consideration of an individual’s ethnic, social, sexual and economic status.
“Both the degree of risk for HIV-1 infection of the person studied and the degree of reactivity of the serum may be of value in interpreting the test” – (Abbott Laboratories HIV Test – EIA)
It is highly unethical to assume that two identical reactions mean different things, based on socio-economic factors and sexual preference, but that seems to be precisely what is being done every day in HIV test labs.
Given the subjective, variable interpretation of HIV tests, how accurate are they at predicting illness? The medical literature makes this very clear:
“Most patients (68 to 89%) from low risk groups who show reactivity on screening tests will have false-positive results… The predictive value of a positive ELISA varies from 2% to 99%....The Western blot method lacks standardization, is cumbersome, and is subjective in interpretation of banding patterns. ”
Steckelberg JM, Cockerill F. Serologic testing for human immunodeficiency virus antibodies. Mayo Clin Proc. 1988;63:373-9.“[I]n low prevalence populations the predictive value [of an HIV test] was 11.1%, while in populations with known HIV-1 infection, the predictive value was 97.1%.”
Abbott Laboratories. HIV Antibody Test. April, 1996.
HIV antibody tests are believed to be somewhere between 2% to 99% accurate, depending on a subjective interpretation of your “risk group,” made by whoever is reading your test.
The result of this lack of medical standards is that if you’re Black, Hispanic, poor, using drugs, in prison, gay or pregnant, then a “nonspecific” test result becomes, in essence, a life sentence. You can be put on toxic drugs and your children can be drugged and taken away from you.
The tests being used on Sean, Dana, Elaine and Liz (see “The Nurse’s Story”), as well as thousands of people around the globe, certainly don’t tell us anything about them that we can’t tell by hearing their life stories: they’re poor, Black, Hispanic, pregnant, they’ve used drugs, and they’ve been exposed to stress and illness.
But even if it is assumed that a non-specific antibody reaction actually represents a virus, there’s still a problem. No one knows how HIV works. As Stevenson points out in Nature, no one has proven how HIV infects a cell, let alone how it causes disease, if, indeed, it does. The hypotheses state that HIV is the primary agent responsible for AIDS, but have yet to fundamentally prove that AIDS is a disease with a single cause.
Meanwhile, researchers of note who have posited alternative disease models that more successfully explain the immune suppression that occurs in AIDS patients, have typically been attacked for dissenting from the mainstream, and are actively kept out of the medical discussion. And so, as far as understanding and treating AIDS is concerned, despite “considerable efforts,” we are only permitted to have “two major hypotheses.”
Stevenson concludes his “Nature” article by acknowledging how little is known about HIV. “[W]hat we know represents only a thin veneer on the surface…” But like most AIDS researchers, he remains stuck to the failed hypothesis. In order to understand HIV better, Stevenson writes, “a permissive, small animal model would be a key experimental tool.”
AIDS researchers, failing to prove the HIV hypothesis accurate, have instead clung onto it stubbornly for 20 years, prescribing extraordinarily toxic drugs to patients in spite of the well-documented inaccuracy of the HIV test. According to Stevenson, they haven’t even done the appropriate experiments in animals before inflicting toxic pharmaceuticals onto the general population.
But this doesn’t seem to bother NIAID, the NIH, Genentech, Glaxo, Pfizer, Harlem Hospital, Beth Israel, Columbia Presbyterian, or any of NY hospitals that feed children to ICC. They don’t need an animal model. They do their experiments on children.
Afterword
The treatment of patients at ICC currently violates every one of the ethical standards for medical experiments set out by international courts after World War 2.
The children at ICC are enrolled in drug trials without their knowledge,
And without the consent of their parents or guardians.
The experiments are neither safe nor necessary.
The drugs used are known to cause disability and death.
Children who refuse the drugs are force fed, then surgically altered.
Is this acceptable behavior? Or do we need another Nuremberg Trial to remind ourselves how to be civilized?
The experience of Mona, Jacklyn and their children is not unique. It is mirrored by patients throughout the United States and across the globe who have made sick by the irrational, profit-driven use of dangerous pharmaceuticals. Informed mothers who try to protect their children from deadly drug therapies are labeled renegades, and risk losing their children to state agencies closely aligned with - and even by funded by - the very companies that produce and sell the drugs.
If this is to stop, it will be up to all of us - citizens, scientists, health advocates, activists, mothers, fathers and family members - to bring this to public attention, to protect the rights of these children, and to remind the medical establishment of their sacred oath: “Primum Non Nocere.” First, Do No Harm.
There are organizations dedicated to protecting human rights and preserving medical and social ethics. If you’re disturbed by this story, let them know about it.
Organization: Amnesty International
Phone / Fax: T (212) 807-8400 / F (212) 463-9193
Address: 322 8th Avenue, New York, NY 10001
Web Address / Email: www.amnestyusa.org / admin-us@aiusa.org
Organization: Physicians Committee for Responsible Medicine
Phone / Fax: T (202) 686-2210 / F (202) 686-2216
Address: 5100 Wisconsin Ave., Suite 400, Washington, DC 20016
Web Address / Email: www.pcrm.org / pcrm@pcrm.org
Organization: Alliance for Human Research Protection
Address: 548 Broadway, 3rd floor, New York, NY 10012
Web Address / Email: http://www.ahrp.org/about/about.html / veracare@rcn.com
Organization: A.C.L.U. New York
Phone / Fax: T (212) 344-3005 / F (212) 344-3318
Address: 125 Broad Street, 17th Floor, New York, NY 10004
Web Address / Email: nyclucrc@capital.net
http://www.nyclu.org/
Organization: N.A.A.C.P.
Phone / Fax: T (877) NAACP-98, 24 Hour Hotline: T (410) 521-4939
Address: 4805 Mt. Hope Drive, Baltimore, Maryland 21215
Web Address / Email: washingtonbureau@naacpnet.org
http://www.naacp.org
Organization: Public Citizen
Phone: T (202) 588-1000
Address: 1600 20th Street, NW, Washington, DC 20009
Web Address / Email: hrg1@citizen.org
http://www.citizen.org
Organization: Prevent Child Abuse New York
Phone / Fax: T (518) 445-127, T 1-800 CHILDREN / F (518) 436-5889
Address: 134 S. Swan St., Albany, NY 12210
Web Address / Email: cdeyss@preventchildabuseny.org
It’s never too late for any doctor to examine what he or she is doing and make a change. Following the leads of Jacklyn Herger and Mona Newberg, we may not only find that a cure for Pediatric AIDS is possible, but that it’s always been possible. We have nothing to lose, and everything to gain by exploring these options.
For the sake of the children at ICC, and the children yet to come – Doctors, it’s time for a new hypothesis.
See the ICC picture gallery.
References:
1) Giraldo Dr. RA. Everybody Reacts Positive on the ELISA Test for HIV. Continuum (London) 1999; 5(5): 8-10.
2) Giraldo, Dr. RA. Tests for HIV are Highly Inaccurate. Posted during the South African Presidential AIDS Advisory Panel, 2000b. http://www.robertogiraldo.com
3) Johnson C. Is anyone really positive? Continuum (London) April/May 1995.
4) Johnson C. Whose Antibodies are They Anyway? Continuum (London), September/October 1996; 4(3):4-5
5) Johnson C. Factors known to cause false-positive HIV antibody test results. Zenger’s Magazine, San Diego, California; September 1996; 8-9. http://www.virusmyth.net
6) Stevenson, Mario. HIV-1 Pathogenesis. Nature Medicine, HIV Special. July 2003. Vol.9, No. 7. 853-861.
7) Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Causer D. The Isolation of HIV: Has it really been achieved? Continuum 1996;4:1s-24s.8.
8) Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Causer D. A critical analysis of the evidence for the isolation of HIV. At Website http://www.virusmyth.com/aids/data/epappraisal.htm 1997.
9) Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, et al. Between the Lines. A Critical Analysis of Luc Montagnier’s Interview Answers to Djamel Tahi. Continuum (London) 1997/8; 5(2):35-45.
10) Scheff, Liam – The AIDS Debate – The Most Controversial Story You’ve Never Heard. Boston’s Weekly Dig. May 7, 2003. ttp://www.altheal.org/texts/liamscheff.htm
11) Lauritsen, John – The AIDS War.
12) Duesberg, P., Koehnlein, C., and Rasnick, D. The chemical bases of the various AIDS epidemics: recreational drugs, anti-viral chemotherapy and malnutrition. J. Biosci., 28: 383-412, 2003.
13) Durack, D. T. Opportunistic infections and Kaposi's sarcoma in homosexual men. The New England Journal of Medicine, 305: 1465-1467, 1981.
14) Oppenheimer, G. M. Causes, cases, and cohorts: The role of epidemiology in the historical construction of AIDS. In: D. M. Fox
(ed.), AIDS: The Making of a Chronic Disease, pp. 49-83. Berkeley: University of California Press, 1992.
15) Jaffe, H. W., Choi, K., Thomas, P. A., Haverkos, H. W., Auerbach, D. M., Guinan, M. E., Rogers, M. F., Spira, T. J., Darrow, W. W., Kramer, M. A., Friedman, S. M., Monroe, J. M., Friedman-Kien, A. E., Laubenstein, L. J., Marmor, M., Safai, B., Dritz, S. K., Crispi, S. J., Fannin, S. L., Orkwis, J. P., Kelter, A., Rushing, W. R., Thacker, S. B., and Curran, J. W. National case-control study of Kaposi's sarcoma and Pneumocystis carinii pneumonia in homosexual men: Part 1, Epidemiologic results. Ann. Intern. Med., 99: 145-151, 1983
16) Papadopulos-Eleopulos E, Turner VF, Papdimitriou JM. Is a Positive Western Blot Proof of HIV Infection? Bio/Technology 1993;11:696-707.
*) Christine Maggiore: “What If Everything You Thought You Knew About AIDS Was Wrong,” http://www.aliveandwell.org
**) Some Continuum magazines : http://perso.wanadoo.fr/esprit-libre/continuum/continuum.htm
Read The Nurse's Story:
Jacklyn Herger is a pediatric AIDS nurse who worked at ICC in the early 90s. In 1996 she began the adoption process for two HIV-positive children from ICC through Catholic Home Bureau In 1998, the girls, Elaine, age six, and Liz, age four, came to live with Herger, her husband and five-year-old daughter as a family. A trained nurse, Herger gave AIDS drugs “by the book.” To her shock and amazement, it was only when she stopped giving the drugs that the girls got better.
Latest news!
(Update 14th July 04)
The New York Press, (NYC's independent weekly) has picked up Liam Scheff's investigation of Pediatric AIDS medical abuse.
The article reports the facts about AIDS drug toxicity, HIV test non-specificity, and exposes the current practice of force-drugging children who refuse their medication through surgically-implanted stomach tubes (g-tubes).
The paper deserves credit for its courage. The NY Press has a large and active letters page. They will, no doubt, receive their share of "fan mail" from the mainstream for publishing this.
Please let them know that their decision to publish this is appreciated, and important to the health and welfare of people everywhere who are fighting medical tyranny.
So many thanks to the NY Press.
Read "Orphans on Trial".
5th July 2004
In January, 2004, I published "The House That AIDS Built." The story was picked up by several international papers, including the New York Post and the UK Guardian, and was reprinted throughout the world on the world wide web.
German journalist Torsten Engelbrecht read the story and formulated a series of questions for Columbia Presbyterian, the hospital which presides over ICC. He was answered by a PR firm. The answers were dishonest and unsatisfactory. What follows is a response to and a dissection of their answers using NIH documents, clinical trials, interview material, Medline articles and Department of Health statistics. Given the material provided here, it is clear that the practice of surgical forced-drugging of HIV positive children with toxic compounds is ongoing, in violation of the rights of wards of the state, and must be addressed immediately.
Read the result of this additional research:
"The ICC Investigation Continues.
Hospital PR firm gives insufficient response to ICC Investigation"Patricia Nell Warren, author of fiction bestsellers like The Front Runner, also writes provocative commentary has recently taken up Liam Scheff's reporting.
Her article "Asking the Questions" is available on http://www.aumag.org/viewfinder/leftMay04.html
What does it mean when a story about possible clinical trial abuses hits the wire, but most news media ignore it? For years, CNN’s Christiane Amanpour has been saying—not on CNN, of course—that courageous reporting is vanishing from the U.S. major media.
March 2004.
Phase I Drug Trials Used Foster Care children in Violation of 45 CFR 46.409 and 21 CFR 50.56
http://www.ahrp.org/ahrpspeaks/HIVkids0304.html
Vera Sharav of the Alliance for Human Research Protection (AHRP) has called for a Federal investigation into Incarnation Children's Center, and the NIH's Pediatric AIDS Clinical Trials program. The AHRP letter contends that Federal Regulations regarding the use of children and wards are being violated.April 2004
London Observer/Guardian Confirms "The House That AIDS Built"
http://observer.guardian.co.uk/international/story/0,6903,1185305,00.html
The incarnation Children's Center story has again been picked up and validated by another major paper - this time by Antony Barnett of the London Observer.New York Post Confirms "The House That AIDS Built"
Liam Scheff investigated and wrote "The House That AIDS Built" throughout 2003, and web-published it in 2004. In early February, 2004, Douglas Montero, a columnist for the NY Post, contacted Scheff after reading the article. Soon after, the Post printed (stole) Scheff's article in a tabloid format rewritten by Montero, without a single mention of Scheff.Two days after the intitial Post cover, Scheff was mentioned in the Post as "a health advocate who investigated ICC and posted his findings on the internet..."
Scheff is indeed a health advocate, but he is also an investigative reporter whose previous work on politics, film and HIV/AIDS has been widely read and praised. Scheff remains hard at work on this and other stories relating to human, medical and civil rights. If you feel so inclined, please contact the NY Post, thanking them for covering this important issue, and reminding them that proper credit should be paid to Scheff and sites like altheal and aras (the Alberta Reappraising AIDS Society), who had the courage to post Scheff's story first, and honestly.
I appreciate you being here.
If you've found the content interesting, useful and maybe even helpful, please consider supporting it through a small paid subscription. While everything here is free, your paid subscription is important as it helps in covering some of the operational costs and supports the continuation of this independent research and journalism work. It also helps keep it free for those that cannot afford to pay.
Please make full use of the Free Libraries.
Unbekoming Interview Library: Great interviews across a spectrum of important topics.
Unbekoming Book Summary Library: Concise summaries of important books.
Stories
I'm always in search of good stories, people with valuable expertise and helpful books. Please don't hesitate to get in touch at unbekoming@outlook.com
For COVID vaccine injury
Consider the FLCCC Post-Vaccine Treatment as a resource.
Baseline Human Health
Watch and share this profound 21-minute video to understand and appreciate what health looks like without vaccination.
I will read the article this evening. But I wanted to say three things. First, you have made an incredible contribution to the world by introducing so many people to Official Stories. Second, I am presently reading it for the 3rd time. Each time I read it I find new nuggets. My goal is to eventually read it 10 times. Third, I’ve been a free subscriber for quite awhile. But I’m going to change that shortly. I have too many paid subscriptions and am letting some of them roll off. Over the past few months your stack has become my favorite non financial related work. You continue to bring forward new and interesting topics each time you post. Time for me to recognize your efforts. Eric.
Can’t talk about AIDS without mentioned Dr. Fauci! If there was a “Demon Lord Hall of Fame,” he’d definitely be in it.
To convince the world of first AIDS and most recently COVID — and to have billions poured into treatments, yep, he’s a first time ballot hall of famer: https://unorthodoxy.substack.com/p/why-it-does-matter