Plenty has been said about Ivermectin. Those of us that are awake (except for Alex Berenson) know that it works, has been withheld from use and also have a general understanding of why they did it.
But I didn’t understand the details of how they blocked Ivermectin until I read Kennedy Jr.’s, The Real Anthony Fauci and I certainly wasn’t aware of the discussion between Dr. Tess Lawrie and Andrew Hill on 13 January 2021. The discussion between them was of such import that Kennedy Jr. dedicated several pages of the book to the transcript. I realised at the time of reading that their discussion was a pivotal moment is the history of the Covid story, a sliding door moment, and remember thinking that I needed to write an article around that transcript. It went onto my to do shelf and unfortunately collected dust there.
This morning I came across this incredible video (above) posted by Ian Clayton and decided to synthesise it with the transcript and other relevant material about Ivermectin.
I recommend you first (or at least) watch the 19 min video above titled A Letter to Andrew Hill.
It will eventually be censored on Facebook and elsewhere which is one of the reasons I’ve chosen to store it in this article.
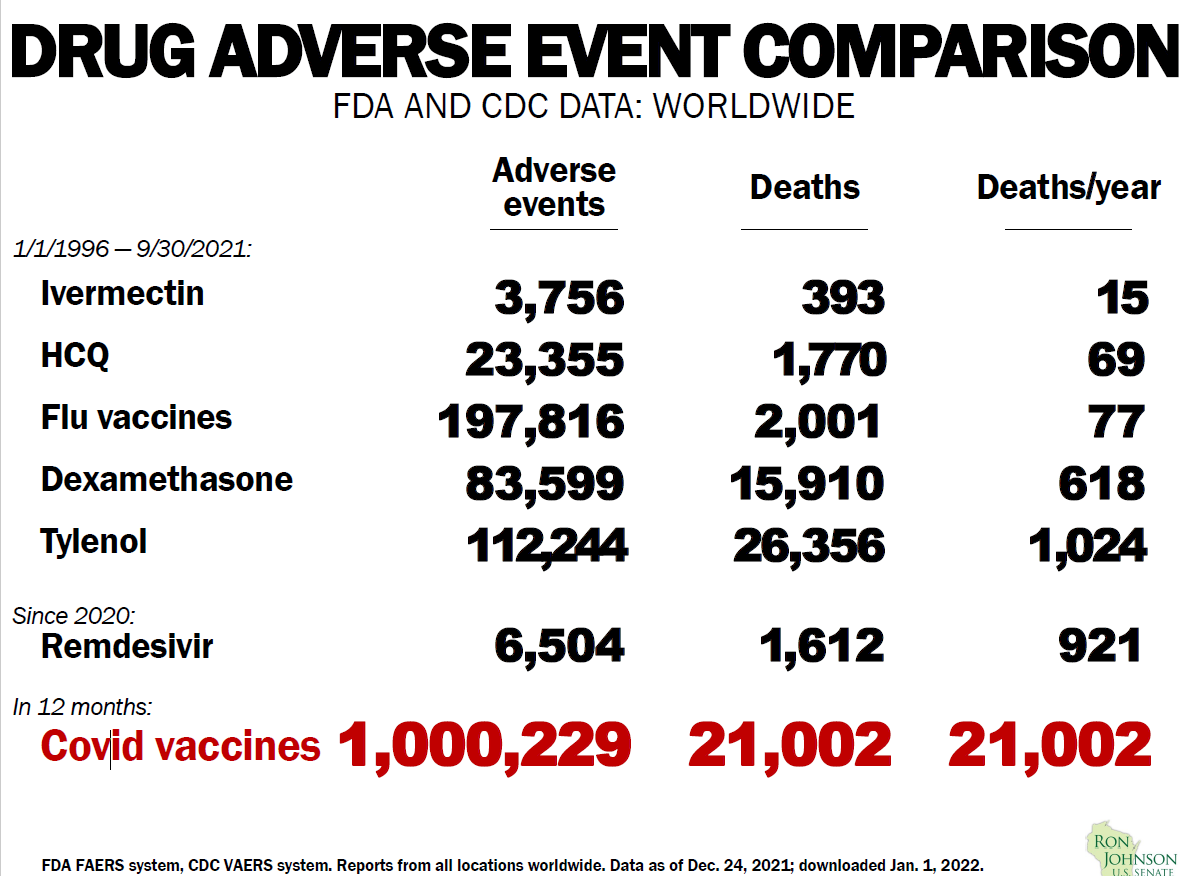
As I was writing this article today I got an email from Igor Chudov’s Substack about yet another study confirming Ivermectin’s value. This one is especially interesting because it’s a head to head against Pharma’s “preferred drug” Remdesivir. Turns out Ivermectin is 70% more effective!! But, honestly we knew that already because we already know that Remdesivir is dangerous and useless, but that’s another story.
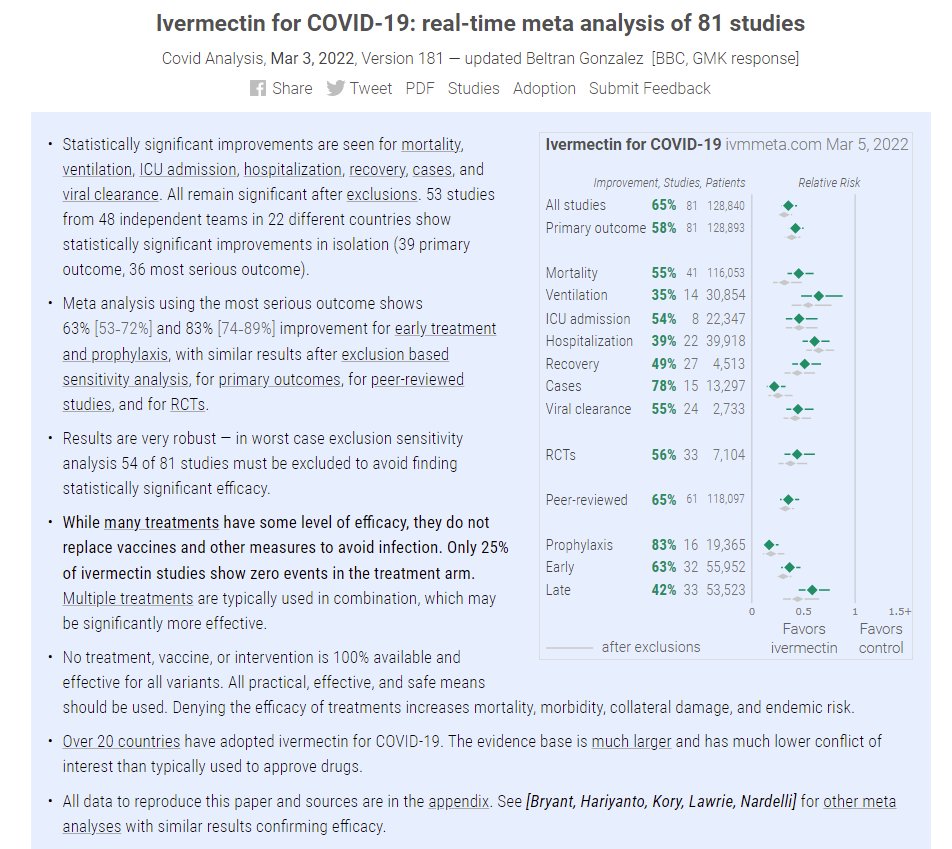
This site keeps track of all the latest evidence and studies on Ivermectin. If anybody has any doubts about the medicine, they should spend some time on this site and see how that maps over what you hear from the BBC of The Guardian.
The decision to prevent us from accessing Ivermectin has killed millions, and the legacy of that decision rolls on in the death and destruction caused by the genetic jabs. It’s reasonable to argue that we might not have ended up with these highly dangerous and highly ineffective genetics rushed out under an EUA, but for the decision to assassinate Ivermectin.
Andrew Hill played a pivotal, arguably key, role in that assassination.
The Ivermectin story, that of withholding cheap, safe and effective drugs from the public, is not a new one.
They (and I am sure you know by now that there is a “they”) have done this before during AIDS. It’s the main reason I am so fascinated with the AIDS story because the template of today’s crisis was built during AIDS where they withheld Bactrim, a cheap and long used antibiotic for several years until they brought the toxic chemo therapy AZT to market. I’ve written a bit about Bactrim here.
According to Callen, “We asked him (Fauci)—no, we begged him —to issue interim guidelines urging physicians to prophylax those patients deemed at high risk for PCP (pneumonia) [with
Bactrim or aerosol pentamidine]. Although it would not have cost the government much to have done so, he (Fauci) steadfastly refused to issue such guidelines. His reason: no data. So, the Catch-22 was complete, and many people died of PCP who didn’t have to.”
When the activists asked Dr. Fauci to at least add AL 721, Peptide D, DHPG, and aerosolized pentamidine to his clinical trials, Dr. Fauci’s refusal was loud: “I can’t do that!” he shouted. “I can’t convene a consensus conference.” The choice, he explained, of which compounds would enter NIAID’s clinical trial pipeline was made, not by public agreement, but by a panel of “independent scientists.” Dr. Fauci did not mention that virtually all the members of his “independent panel” were pharmaceutical PIs, with ties to NIAID and Burroughs Wellcome.
In today’s story they withheld HCQ and even more importantly Ivermectin (IVE) until they got the ineffective and dangerous Remdesivir, and the genetics, to market.
I find it hard to explain how significant the Ivermectin obstruction has been. Dr. Tess Lawrie in the video above does a wonderful job. But in June of 2021 I used the following analogy:
Imagine that someone has a heart attack on an aeroplane, and there are 5 doctors on the flight, all of them as it turns out are heart specialists. They start running towards the patient to help but get crash tackled by air hostesses and onboard airline security, even the co-pilot jumps in to punch the doctors. Anyway, the patient dies and several of the doctors lose their license for trying to help. Turns out the reason is that the airline has also invested in a new heart treatment and that is the only treatment it will allow its passengers. The treatment involves heavy machinery that is at the airport, so the patient must wait until landing.
Do you think that the airline, its employees and hired help are involved in a Criminal Obstruction? I do.
If you need any evidence at all that there is structural, centralised malfeasance at play, look no further than Ivermectin and this subject generally.
On the question of who Dr. Tess Lawrie is, I’m simply going to refer you to Margaret Anna Alice’s wonderful profile of her from Dec. 2021.
I watched this in August 2021 and knew that the question of Ivermectin was finally asked and answered. What I didn’t understand at that point was how important it was to kill Ivermectin so as to justify the Emergency Use Authorization (EUA). Dr. Lawrie makes that point very clearly in the video at the top (A Letter to Andrew Hill).
Dr. Peter McCullough said this on Rogan:
Rogan
Now again, though, why do you think hydroxychloroquine was demonized? Why do you think that it was, especially so early on in Australia? It can’t be universal incompetence across the board. So one of the things that’s interesting about Ivermectin is it’s not demonized worldwide. It’s distributed widely in other countries, and it’s shown some effectiveness.
McCullough
Absolutely. Ivermectin now is first line in Japan. It’s attributed to crushing the curves in Mexico.
In Peru absolutely crushed the curves in India. We’ve been in close communication with them. Ivermectin is an interesting drug and I know you’ve reviewed it in depth on this show, so I’ll leave it to experts like Dr. Kory and others there, but I use it every day in my practice I have no problems with Ivermectin. It is safe and effective. It’s been a Nobel Prize awarded in 2015 for Ivermectin.
Dr. Robert Malone, on Rogan, said this is response to Joe’s question about Ivermectin:
Rogan
Why do you think that is? What do you think is going on with the pushback on Ivermectin?
Malone
So, it’s not just Ivermectin, it’s hydroxychloroquine. And just to put a marker on that, there’s good modeling studies that probably half a million excess deaths have happened in the United States through the intentional blockade of early treatment by the US government. Half a million. That is a well-documented number. And it’s a combination of hydroxychloroquine and Ivermectin. Now when you ask me why you’re asking me to get into somebody’s head, what I can say as a scientist is what I observe, the behaviors, the actions, the correspondence, these bizarre things like, don’t you know it’s a horse drug, Y’all, which is amazingly pejorative. I live in Virginia. Okay, I can tell you the people around me, I live in a rural county, and I raise horses. That was deeply offensive to use that language in that way. But there’s clearly been an intentional push. And Zeb Zelenko, who’s a buddy, the guy that came out with the original protocol, the Zelenko Protocol, and was the one, by the way, that wrote the letter to Trump advocating for hydroxychloroquine. One kind of important to put that together. He’s put together a great little video clip in which he clearly documents the conspiracy between Janet Woodcock and Rick Bright to make it so that physicians could not administer hydroxychloroquine outside of the hospital.
-
It is bizarre that Merck would come out with these explicit statements about the safety of Ivermectin. Both Ivermectin and Hydroxy are on the WHO list of essential medicines. They have been administered for millions and millions of doses. They’re among the safest medicines we know when administered within this acceptable window. Pharmaceutical window. Ivermectin is even safer than hydroxy. So, Merck coming out out of the blue and saying Ivermectin isn’t safe is really inexplicable. Now another thing is that I sit on the Active Committee for Drugs as an observer. What is the Active Committee? This is the NIH committee that’s guiding the clinical trials for these various repurposed and novel drugs. I saw listened to heard witnessed the representative of Merck that’s on the committee because the committee is full of pharmaceutical representatives, even though it’s an NIH public committee explicitly attack the decision for the federal government to test Ivermectin. She said, there’s no reason to do this…But there is clearly a concerted effort on the part of multiple players in the pharmaceutical industry in accordance with the federal government to kill Ivermectin as a potential alternative early treatment strategy.
The following excerpt from The Real Anthony Fauci looks at the details of how they sabotaged Ivermectin including the full transcript of the discussion Dr. Tess Lawrie had with Andrew Hill.
The Real Anthony Fauci
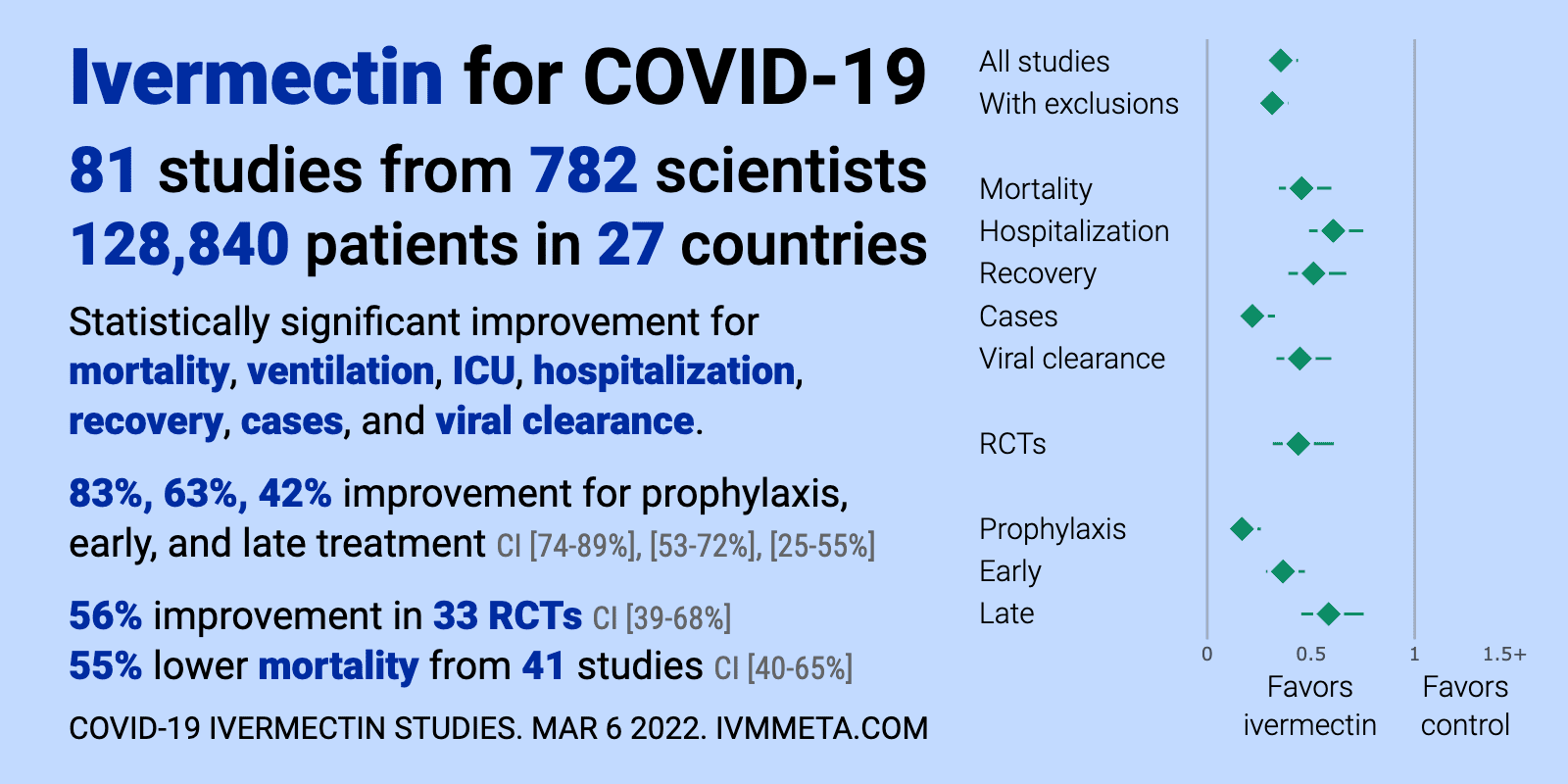
The massive and overwhelming evidence in favor of ivermectin includes scientist Dr. Tess Lawrie’s highly regarded, peer-reviewed meta-analysis.
Dr. Lawrie assessed 15 trials, finding a cumulative benefit of IVM in reducing deaths of 62 percent. Although the data quality of the ivermectin for prevention studies was less strong, they showed that ivermectin prophylaxis reduced COVID infections by 86 percent.
Dr. Lawrie, a world-renowned data researcher and scientific consultant, is an iconic eminence among global public health scientists and agencies. The Desert Review has deemed her “The Conscience of Medicine” because of her reputation for competence, precision, and integrity. Lawrie’s consulting group, the Evidence-Based Medicine Consultancy, Ltd. performs the scientific reviews that develop and support guidelines for global public health agencies, including the WHO and European governments, as well as international scientific and health consortia like the Cochrane Collaboration. Her clients have included a retinue of virtually all the larger government regulators now involved in the suppression of IVM and other repurposed drugs.
At the end of December 2000, Dr. Lawrie happened on a YouTube video of Pierre Kory’s Senate testimony on ivermectin. Her interest piqued, Dr. Lawrie conducted a
“pragmatic rapid review” between Christmas and New Year’s to validate the 27 studies from the medical literature that Kory cited, assessing each of them for quality and power.
“After a week, I realized it was a go. IVM’s safety was well- established as a widely used dewormer,” she told me. “I was startled by the magnitude of its benefits. Its efficacy against COVID was consistently clear in multiple studies. I thought that all these people were dying and this was a moral obligation— this drug should have been rolled out.” Dr. Lawrie dispatched an urgent letter to British Health Minister Matt Hancock on January 4 with her Rapid Review attached. She never heard back from Hancock. But in a suspicious coincidence, someone leaked a meta-review by WHO researcher Andrew Hill to the Daily Mail. Three days later, Hill posted a preprint of his study. In the one month since he testified enthusiastically beside Dr. Kory in favor of ivermectin before the January 13 NIH panel, Hill had made a neck-wrenching volte face. Cumulatively, the seven studies in Hill’s original meta-review still showed a dramatic reduction in hospitalizations and deaths among patients receiving IVM. The leaked version of Hill’s meta-review included all the same papers that formerly supported his gung-ho promotion of IVM as a miraculous cure for COVID. Hill had altered only his conclusions. Now he claimed that those studies comprised a low quality of evidence, and so although they yielded a highly positive result, Hill assigned the result a “low certainty.” He could then declare that WHO should not recommend IVM without first performing long-term, randomized placebo-controlled studies that would require many months if not longer. “Someone got to him,” suggests Kory. “Someone sent him the memo. Andrew Hill has been captured by some really dark forces.”
On January 7, Dr. Lawrie summarized the overwhelming evidence from her Rapid Review in a video directed at British Prime Minister Boris Johnson, urging him to break the logjam and roll out IVM immediately. Her video, says Dr. Kory, was “absolutely convincing.” She forwarded the video appeal to the British and South African Prime Ministers on January 7. She heard nothing from either.
On January 13, 2021, Dr. Lawrie used her convening power to assemble an invitation-only symposium of twenty of the world’s leading experts, including researchers, physicians, patient advocates, and government consultancy advisers, to review her meta-analysis and make evidence-based recommendations on the use of ivermectin to prevent and treat COVID-19. She called the conference the British ivermectin Recommendation Development (BIRD) study.
“Tess Lawrie did exactly what WHO should have done,” says Dr. Kory. “She made a thorough, open, and transparent review of all the scientific evidence.”
During the daylong conference, the conferees reviewed each study in Dr. Lawrie’s rapid meta-review, agreeing that the evidence supported an immediate rollout. Before adjourning, Dr. Lawrie and the scientific panel committed to conducting a full- scale Cochrane-style meta-review of all the scientific literature. Due to the mortal urgencies, they pledged to reconvene in a much larger group on January 14.
In the meantime, Dr. Lawrie managed to reach Andrew Hill by phone on January 6, two days after the Daily Mail leaked his meta-review. She informed him that some of the leading lights of science had agreed to collaborate on the Cochrane-style meta-review, and she proposed that Hill should join the effort as a collaborator. She offered to share her data with Hill and, after the call, she sent him her spreadsheets. Dr. Lawrie had coordinated many Cochrane Reviews for WHO and was indisputably among the world’s ranking experts in systematically reviewing study data. Dr. Lawrie invited Hill to co-author the Cochrane Review and to attend the next BIRD meeting on January 13. It was an exciting opportunity. Under normal circumstances, Hill should have pounced on this chance to serve as lead author with some of the world’s most prestigious researchers in creating a professional, bulletproof Evidence-to-Decision framework for the WHO. He was nevertheless noncommittal. He did agree to review Dr. Lawrie’s spreadsheet.
Dr. Lawrie and her colleagues launched a marathon effort to conduct a brand new review of all published studies in the medical literature from scratch, assessing each for power and bias. She presented her draft to the exclusive BIRD group in mid-January. All agreed that the common-sense approach was to release ivermectin. She submitted the protocol to Cochrane for external scientific review.
British and Scandinavian scientists founded the Cochrane Collaboration in 1993 to address pharmaceutical industry corruption that had become pervasive in clinical trials for new drugs. Today, the Cochrane Collaboration is a coalition of 30,000 independent scientists and 53 large research institutions who volunteer to routinely review industry data using evidence- based science to advise regulatory agencies.60 Cochrane seeks to restore integrity and standardized scientific methodologies to the crooked realm of drug development trials. Cochrane uses standardized parameters and rigorous methodologies for evaluating evidence. Cochrane reviewers systematically assess the power of each individual study within the meta-review, interpreting data to identify and discount for bias, and to score each study as “high,” “moderate,” or “low” certainty evidence and to determine whether it’s acceptable to pool the data in a single meta-review.
Dr. Lawrie knew that to make its ivermectin determination, WHO would rely on Hill’s study and another study from McMaster University known as the “Together Trial.” McMaster was hopelessly and irredeemably conflicted. NIH gave McMaster $1,081,541 in 2020 and 2021. A separate group of McMaster University scientists was, at that time, engaged in developing their own COVID vaccine—an effort that would never pay dividends if WHO recommended ivermectin as Standard of Care. The Bill and Melinda Gates Foundation was funding the massive “Together Trial” testing ivermectin, HCQ, and other potential drugs against COVID, in Brazil and other locations. Critics accused Gates and the McMaster researchers of designing that study to make ivermectin fail. Among other factors, the study targeted a population that was already heavily utilizing ivermectin, creating a confounding variable (placebo recipients could obtain over the counter ivermectin) that would clearly hide efficacy. McMaster University researchers would certainly know that a positive recommendation for IVM would cost their university hundreds of millions. The Together Trial organizer was Gates’ trial designer, Ed Mills, a scientist with heavy conflicts with Pharma and a reputation as a notorious industry biostitute.
Dr. Lawrie knew that the only way to salvage the WHO Guidelines and produce a high-quality scientific study was to persuade Mills to do a full-scale Cochrane Collaboration meta- analysis. The following week, she spoke to Hill again, this time by Zoom.
The Zoom call was recorded.
During her first conversation with Hill, Dr. Lawrie had concluded that the techniques that Hill employed throughout his meta-review were “deeply flawed,” and that Hill lacked the experience to perform a systematic review or a meta-analysis: “I was surprised he had been given the job.”
In fact, the transcript of her January 13 conversation suggests that Hill was completely unfamiliar with the requirements of a systematic review, which requires researchers to evaluate and score each study using uniform criteria to assess power and the risk of bias, and to conduct a “sensitivity analysis” to exclude studies with high risk of bias. This kind of review necessarily judges the reliability of the authors of each participating study. The Cochrane reviewers must be prepared to make harsh judgments about the work quality, integrity, and potential prejudices of each listed co-author of all the studies included in their review, based in part on their individual competence, and the financial conflicts of interest potentially affecting each researcher. But Hill, bizarrely, had included the names of all the authors of all of his seven accumulated studies on the list of the co-authors of his meta-review. “That’s the equivalent of asking the catcher in a baseball team to also play the umpire,” says Dr.
Kory. “No one with any familiarity with the game would make that mistake. Hill was supposed to be judging these authors. Instead, he treated them as his collaborators.”
Dr. Lawrie gently informed Hill that that was “irregular for a meta-analysis,” adding, “When you do a systematic review, you usually don’t include the authors of the studies because that inherently biases your conclusions. It’s got to be independent.”
Dr. Lawrie explained that Hill’s paper, in addition to listing as co-authors the researchers whose work he was supposed to be evaluating, makes no pretense of systematically grading evidence according to standardized protocols. Those deficiencies make it utterly useless, she explained, for providing “clinical guidelines to the WHO.” Furthermore, Hill’s meta- review looked at only one outcome, the deaths of COVID patients, which was only a small subset of the criteria and endpoints in the studies he had analyzed. She told Hill: “You don’t just do a meta-analysis … when there’s all those other outcomes that you didn’t even meta-analyze. You just meta- analyzed the death outcome [using only a fraction of the available evidence], and then [said], ‘Oh, we need more studies.’”
Dr. Lawrie asked Hill to explain his U-turn on ivermectin, which his own analysis found overwhelmingly effective. “How can you do this?” she inquired politely. “You are causing irreparable harm.”
Hill explained that he was in a “tricky situation,” because his sponsors had put pressure on him. Hill is a University of Liverpool virologist who serves as an advisor to Bill Gates and the Clinton Foundation. “He told me his sponsor was Unitaid.” Unitaid is a quasi-governmental advocacy organization funded by the BMGF and several European countries—France, the United Kingdom, Norway, Brazil, Spain, the Republic of Korea, and Chile—to lobby governments to finance the purchase of medicines from pharmaceutical multinationals for distribution to the African poor. Its primary purpose seems to be protecting the patent and intellectual property rights of pharmaceutical companies—which, as we shall see, is the priority passion for Bill Gates—and to insure their prompt and full payment. About 63 percent of its funding comes from a surtax on airline tickets. The Bill & Melinda Gates Foundation holds a board seat and chairs Unitaid’s Executive Committee, and the BMGF has given Unitaid $150 million since 2005. Various Gates-funded surrogate and front organizations, like Global Fund, Gavi, and UNICEF also contribute, as does the pharmaceutical industry. The BMGF and Gates personally own large stakes in many of the pharmaceutical companies that profit from this boondoggle. Gates also uses Unitaid to fund corrupt science by tame and compromised researchers like Hill that legitimizes his policy directives to the WHO. Unitaid gave $40 million to Andrew Hill’s employer, the University of Liverpool, four days before the publication of Hill’s study.
Hill, a PhD, confessed that the sponsors were pressuring him to influence his conclusion. When Dr. Lawrie asked who was trying to influence him, Hill said, “I mean, I, I think I’m in a very sensitive position here… .”
Dr. Tess Lawrie, MD, PhD: “Lots of people are in sensitive positions; they’re in hospital, in ICUs dying, and they need this medicine.”
Dr. Hill: “Well… .”
Dr. Tess Lawrie: “This is what I don’t get, you know, because you’re not a clinician. You’re not seeing people dying every day. And this medicine prevents deaths by 80 percent. So 80 percent of those people who are dying today don’t need to die because there’s ivermectin.”
Dr. Andrew Hill: “There are a lot, as I said, there are a lot of different opinions about this. As I say, some people simply… .”
Dr. Tess Lawrie: “We are looking at the data; it doesn’t matter what other people say. We are the ones who are tasked with … look[ing] at the data and reassur[ing] everybody that this cheap and effective treatment will save lives. It’s clear. You don’t have to say, well, so-and-so says this, and so-and-so says that. It’s absolutely crystal clear. We can save lives today. If we can get the government to buy ivermectin.”
Dr. Andrew Hill: “Well, I don’t think it’s as simple as that, because you’ve got trials… .”
Dr. Tess Lawrie: “It is as simple as that. We don’t have to wait for studies … we have enough evidence now that shows that ivermectin saves lives, it prevents hospitalization. It saves the clinical staff going to work every day, [and] being exposed. And frankly, I’m shocked at how you are not taking responsibility for that decision. And you still haven’t told me who is [influencing you]? Who is giving you that opinion? Because you keep saying you’re in a sensitive position. I appreciate you are in a sensitive position, if you’re being paid for something and you’re being told [to support] a certain narrative … that is a sensitive position. So, then you kind of have to decide, well, do I take this payment? Because in actual fact, [you] can see [your false] conclusions … are going to harm people. So maybe you need to say, I’m not going to be paid for this. I can see the evidence, and I will join the Cochrane team as a volunteer, like everybody on the Cochrane team is a volunteer. Nobody’s being paid for this work.”
Dr. Andrew Hill: “I think fundamentally, we’re reaching the [same] conclusion about the survival benefit. We’re both finding a significant effect on survival.”
Dr. Tess Lawrie: “No, I’m grading my evidence. I’m saying I’m sure of this evidence. I’m saying I’m absolutely sure it prevents deaths. There is nothing as effective as this treatment. What is your reluctance? Whose conclusion is that?” Hill then complains again that outsiders are influencing him.
Dr. Tess Lawrie: “You keep referring to other people. It’s like you don’t trust yourself. If you were to trust yourself, you would know that you have made an error and you need to correct it because you know, in your heart, that this treatment prevents death.”
Dr. Andrew Hill: “Well, I know, I know for a fact that the data right now is not going to get the drug approved.”
Dr. Tess Lawrie: “But, Andy—know this will come out … It will come out that there were all these barriers to the truth being told to the public and to the evidence being presented. So please, this is your opportunity just to acknowledge [the truth] in your review, change your conclusions, and come on board with this Cochrane Review, which will be definitive. It will be the review that shows the evidence and gives the proof. This was the consensus on Wednesday night’s meeting with 20 experts.” Hill protests that NIH will not agree to recommend IVM.
Dr. Tess Lawrie: “Yeah, because the NIH is owned by the vaccine lobby.”
Dr. Andrew Hill: “That’s not something I know about.”
Dr. Tess Lawrie: “Well, all I’m saying is this smacks of corruption and you are being played.”
Dr. Hill: “I don’t think so.”
Dr. Tess Lawrie: “Well then, you have no excuse because your work in that review is flawed. It’s rushed. It is not properly put together.” Dr. Lawrie points out that Hill’s study ignores a host of clinical outcomes that affect patients.
She scolds Hill for ignoring the beneficial effects of IVM as prophylaxis, its effect on speed to PCR negativity, on the need for mechanical ventilation, on reduced admissions to ICUs, and other outcomes that are clinically meaningful.
She adds, “This is bad research … bad research. So, at this point, I don’t know … you seem like a nice guy, but I am really, really worried about you.”
Dr. Andrew Hill: “Okay. Yeah. I mean, it’s, it’s a difficult situation.”
Dr. Tess Lawrie: “No, you might be in a difficult situation. I’m not, because I have no paymaster. I can tell the truth … How can you deliberately try and mess it up … you know?”
Dr. Andrew Hill: “It’s not messing it up. It’s saying that we need, we need a short time to look at some more studies.”
Dr. Tess Lawrie: “So, how long are you going to let people carry on dying unnecessarily—up to you? What is, what is the timeline that you’ve allowed for this, then?”
Dr. Andrew Hill: “Well, I think … I think that it goes to WHO and the NIH and the FDA and the EMEA. And they’ve got to decide when they think enough’s enough.”
Dr. Tess Lawrie: “How do they decide? Because there’s nobody giving them good evidence synthesis, because yours is certainly not good.”
Dr. Andrew Hill: “Well, when yours comes out, which will be in the very near future … at the same time, there’ll be other trials producing results, which will nail it with a bit of luck. And we’ll be there.”
Dr. Tess Lawrie: “It’s already nailed.”
Dr. Andrew Hill: “No, that’s, that’s not the view of the WHO and the FDA.”
Dr. Tess Lawrie: “You’d rather… risk loads of people’s lives. Do you know if you and I stood together on this, we could present a united front and we could get this thing. We could make it happen. We could save lives; we could prevent [British National Health Service doctors and nurses] people from getting infected. We could prevent the elderly from dying.”
Dr. Tess Lawrie: “These are studies conducted around the world in several different countries. And they’re all saying the same thing. Plus there’s all sorts of other evidence to show that it works. Randomized controlled trials do not need to be the be- all and end-all. But [even] based on the randomized controlled trials, it is clear that ivermectin works… It prevents deaths and it prevents harms and it improves outcomes for people … I can see we’re getting nowhere because you have an agenda, whether you like it or not, whether you admit to it or not, you have an agenda. And the agenda is to kick this down the road as far as you can. So … we are trying to save lives. That’s what we do. I’m a doctor and I’m going to save as many lives as I can. And I’m going to do that through getting the message [out] on ivermectin… . Okay. Unfortunately, your work is going to impair that, and you seem to be able to bear the burden of many, many deaths, which I cannot do.” Then she asks again.
Dr. Tess Lawrie: “Would you tell me? I would like to know who pays you as a consultant through WHO.”
Dr. Andrew Hill: “It’s Unitaid.”
Dr. Tess Lawrie: “All right. So who helped to … ? Whose conclusions are those on the review that you’ve done? Who is not listed as an author? Who’s actually contributed?”
Dr. Andrew Hill: “Well, I mean, I don’t really want to get into, I mean, it … Unitaid … .”
Dr. Tess Lawrie: “I think that … It needs to be clear. I would like to know who, who are these other voices that are in your paper that are not acknowledged. Does Unitaid have a say? Do they influence what you write?”
Dr. Andrew Hill: “Unitaid has a say in the conclusions of the paper. Yeah.”
Dr. Tess Lawrie: “Okay. So, who is it in Unitaid, then? Who is giving you opinions on your evidence?”
Dr. Andrew Hill: “Well, it’s just the people there. I don’t … .”
Dr. Tess Lawrie: “So they have a say in your conclusions.”
Dr. Andrew Hill: “Yeah.”
Dr. Tess Lawrie: “Could you please give me a name of someone in Unitaid I could speak to, so that I can share my evidence and hope to try and persuade them to understand it?”
Dr. Andrew Hill: “Oh, I’ll have a think about who to, to offer you with a name…. But I mean, this is very difficult because I’m, you know, I’ve, I’ve got this role where I’m supposed to produce this paper and we’re in a very difficult, delicate balance….”
Dr. Lawrie interjects: “Who are these people? Who are these people saying this?”
Dr. Andrew Hill: “Yeah … it’s a very strong lobby …”
Dr. Tess Lawrie: “Okay. Look I think I can see [we’re] kind of [at] a dead end, because you seem to have a whole lot of excuses, but, um, you know, that to, to justify bad research practice. So I’m really, really sorry about this, Andy. I really, really wish, and you’ve explained quite clearly to me, in both what you’ve been saying and in your body language that you’re not entirely comfortable with your conclusions, and that you’re in a tricky position because of whatever influence people are having on you, and including the people who have paid you and who have basically written that conclusion for you.”
Dr. Andrew Hill: “You’ve just got to understand I’m in a difficult position. I’m trying to steer a middle ground and it’s extremely hard.”
Dr. Tess Lawrie: “Yeah. Middle ground. The middle ground is not a middle ground… [Y]ou’ve taken a position right to the other extreme calling for further trials that are going to kill people. So this will come out, and you will be culpable. And I can’t understand why you don’t see that, because the evidence is there and you are not just denying it, but your work’s actually actively obfuscating the truth. And this will come out. So I’m really sorry … As I say, you seem like a nice guy, but I think you’ve just kind of been misled somehow.” Hill promised he would do everything in his power to get ivermectin approved if she would give him six weeks.
Dr. Andrew Hill: “Well, what I hope is that this, this stalemate that we’re in doesn’t last very long. It lasts a matter of weeks. And I guarantee I will push for this to last for as short amount of time as possible.”
Dr. Tess Lawrie: “So, how long do you think the stalemate will go on for? How long do you think you will be paid to [make] the stalemate… go on?”
Dr. Andrew Hill: “From my side. Okay … I think end of February, we will be there six weeks.”
Dr. Tess Lawrie: “How many people die every day?”
Dr. Andrew Hill: “Oh, sure. I mean, you know, 15,000 people a day.”
Dr. Tess Lawrie: “Fifteen thousand people a day times six weeks … Because at this rate, all other countries are getting ivermectin except the UK and the USA, because the UK and the USA and Europe are owned by the vaccine lobby.”
Dr. Andrew Hill: “My goal is to get the drug approved and to do everything I can to get it approved so that it reaches the maximum… .”
Dr. Tess Lawrie: “You’re not doing everything you can, because everything you can would involve saying to those people who are paying you, ‘I can see this prevents deaths. So I’m not going to support this conclusion anymore, and I’m going to tell the truth.’”
Dr. Andrew Hill: “What, I’ve got to do my responsibilities to get as much support as I can to get this drug approved as quickly as possible.”
Dr. Tess Lawrie: “Well, you’re not going to get it approved the way you’ve written that conclusion. You’ve actually shot yourself in the foot, and you’ve shot us all in the foot. All of … everybody trying to do something good. You have actually completely destroyed it.”
Dr. Andrew Hill: “Okay. Well, that’s where we’ll, I guess we’ll have to agree to differ.”
Dr. Tess Lawrie: “Yeah. Well, I don’t know how you sleep at night, honestly.”
At the conclusion of the January 14 BIRD conference, Dr. Lawrie delivered a monumental closing address that should be recorded among the most important speeches in the annals of medical history. Dr. Lawrie spoke out at considerable personal risk, since her livelihood and career largely rely on the very agencies she targeted for criticism.
Dr. Lawrie began by endorsing the miraculous efficacy of IVM.
Had ivermectin been employed in 2020 when medical colleagues around the world first alerted the authorities to its efficacy, millions of lives could have been saved, and the pandemic with all its associated suffering and loss brought to a rapid and timely end.
Dr. Lawrie told the audience that the suppression of ivermectin was a signal that Pharma’s pervasive corruption had turned a medical cartel against patients and against humanity.
The story of ivermectin has highlighted that we are at a remarkable juncture in medical history. The tools that we use to heal and our connection with our patients are being systematically undermined by relentless disinformation stemming from corporate greed. The story of ivermectin shows that we as a public have misplaced our trust in the authorities and have underestimated the extent to which money and power corrupts.
Dr. Lawrie called for reform of the method used to analyze scientific evidence.
They who design the trials and control the data also control the outcome. So, this system of industry-led trials needs to be put to an end. Data from ongoing and future trials of novel COVID treatments must be independently controlled and analyzed. Anything less than total transparency cannot be trusted.
Dr. Lawrie called out the corruption of modern medicine by Big Pharma and other interests and attributed the barbaric suppression of IVM to the single-minded obsession with more profitable vaccines.
Since then, hundreds of millions of people have been involved in the largest medical experiment in human history. Mass vaccination was an unproven novel therapy. Hundreds of billions will be made by Big Pharma and paid for by the public. With politicians and other nonmedical individuals dictating to us what we are allowed to prescribe to the ill, we as doctors have been put in a position such that our ability to uphold the Hippocratic oath is under attack.
She hinted at Gates’ role in the suppression.
At this fateful juncture, we must therefore choose: will we continue to be held ransom by corrupt organizations, health authorities, Big Pharma, and billionaire sociopaths, or will we do our moral and professional duty to do no harm and always do the best for those in our care? The latter includes urgently reaching out to colleagues around the world to discuss which of our tried and tested safe older medicines can be used against COVID.
Never before has our role as doctors been so important, because never before have we become complicit in causing so much harm.
Finally, Dr. Lawrie suggested that physicians form a new World Health Organization that represents the interests of the people, not corporations and billionaires, a people-centered organization.
* * *
On October 1, 2021, Hill resurfaced on Twitter touting his upcoming lecture, ironically titled, “Effects of Bias and Potential Medical Fraud in the Promotion of Ivermectin.” Says Pierre Kory in disgust, “Andrew is apparently making a living now accusing the doctors and scientists who support ivermectin of medical fraud.” Dr. Kory adds, “Hill and his backers are some of the worst people in human history. They are responsible for the deaths of millions.”









The assassination of Ivermectin and the death of millions