


Tetanus the “T” in DTP: Rusty Nails, Latex, Gorillas and Sterilisation
I miss my 2019 ignorant innocence. But, as I am discovering, it was a deadly innocence.


[Note: Take 2. Embarrassingly a part of the previous edition referred to the weight of all the doses incorrectly that lead to my golf ball analogy. I have now deleted the incorrect passage. Sorry about that! Even amateurs make mistakes!]
My story that began with waking up to the dangers and lies of Covid jabs has morphed into a journey to understand what else they have lied to me about and what is true about what we injected into our kids all those years ago.
The point of these posts is threefold; they force me to learn up on the subject, they are a journal entry to remind me of this time after much has faded from my memory and most importantly they are a message in a bottle to anyone who reads them to teach them a thing or two about a subject they may know nothing about (just as I was ignorant once) and with that sow the seed of curiosity so that they may investigate further and make better decisions than I made when I was asleep at the wheel and in an MGM Triad manufactured trance, obeying all vaccination orders and letting them do as they pleased with my kids.
So, if you have or are about to have a baby, I hope these posts help you to make better decisions than I did.
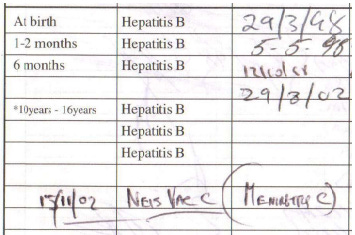
I went back to look at the schedule of shots we gave to our kids:
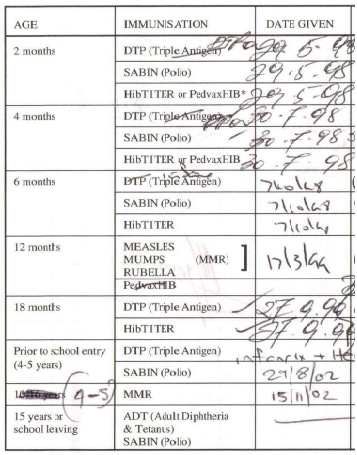
In summary they are:
DTP – Diphtheria, Tetanus and Pertussis
Polio (Sabin)
Hibtiter – Heamophilus Influenza Type B
MMR – Measles, Mumps and Rubella
Meningitis C
So, on my count 23 doses for 11 diseases.
Plus, Vitamin K which is its own story taking us to 24 doses for 12 diseases/conditions.
So, presented in a simpler way:
1. Vitamin K
2. Hepatitis B
3. Diphtheria
4. Tetanus
5. Pertussis (Whooping cough)
6. Polio
7. Influenza Type B
8. Measles
9. Mumps
10. Rubella
11. Meningitis C
12. HPV
I’ve written my “messages in a bottle” about HPV and Hepatitis B, and I’m gradually going to write something about all the others as I wrap my head around all of this.
This post is about Tetanus.
Let’s get some terminology straight first. This from the Terminology section of Dissolving Illusions.
DTP
Diphtheria, Tetanus, Pertussis vaccine that used the whole bacterial cell after it was killed. This was the original version of the pertussis vaccine that was highly antigenic but more problematic from a safety standpoint. This vaccine is often termed the whole cell vaccine. It is still used in developing countries.
DTaP
Diphtheria, Tetanus, acellular Pertussis vaccine. The pertussis portion of these vaccines does not use the whole cell but contains the pertussis toxin either alone or in combination with pieces of other virulence factors from the cell. These are the vaccines used in the United States, the United Kingdom, and most of Europe today. They are thought to be much safer but are far less antigenic. They are also more expensive.
So, even though it is described in the schedule above as DTP I’m pretty sure it’s referring to DTaP.
But for the purposes of this article, it’s a distinction without a difference.
I’ve become more of a first principles thinker than I ever used to be, and with that in mind, what does the word “vaccine” really mean, it’s simply a word that has been given “holy” status to describe a combination of chemicals and ingredients. Nothing more. The vial is a chemical stew, no more and no less. So, what’s in the Tetanus brew?
According to this Australian government site the category of ingredients in DTP vaccines available in Australia are:
· Albumin/serum
· Aluminium compounds
· Bovine exposure during manufacturing
· Formaldehyde
· Glutaraldehyde
· Latex/natural rubber
· Neomycin
· Phenoxyethanol
· Polymyxin
· Polysorbate or sorbitol
· Streptomycin
· Yeast
Let’s start off by saying that I don’t know what all these words mean, but my gut feel suggests that unless it is absolutely necessary, and I will talk about necessity later, I don’t want all these foreign agents floating around in my body or anyone else’s body for that matter.
Why the fuck would I want “latex” or “formaldehyde” in me UNLESS IT WAS ABSOLUTELY NECESSARY?
Also, I need to know that they have been tested thoroughly and honestly for safety. Well, the corrupting of placebo test groups means that they haven’t.
Only God knows what flooding your baby’s system with all this junk means over their life, and it’s quite possible that even God doesn’t know. What could be a more complex system than the perfectly fine tuned human body, and what are the odds that injecting these foreign agents into the system are NET POSITIVE. I’ve written about the foreign agent idea in my Cane Toad article.
I wrote a bit about Polysorbate here and referred to a longer article about Polysorbate here.
The Real Anthony Fauci got the ball rolling in understanding vaccine industry malfeasance and now I’m in Candace Owens’ slipstream as she produces her wonderful Shot In The Dark series.
Tetanus has been on my mind ever since I read the Fauci book where Kennedy Jr. discusses in ample detail the “lacing” of Tetanus vaccines for African women. That excerpt is later in this post.
Having said all of that, I listened to Candace’s latest episode and heard her talking about Tetanus (from a different angle) and I thought the two different threads are worthy of an article.
Episode 7: Suddenly Infants Dying! (DTAP Beginnings)
The episode starts off with a discussion of SIDS (Sudden Infant Death Syndrome) and as I was listening to her my mind wandered to the current “Died Suddenly” headlines that are everywhere and I realised it’s the same word “Sudden” and the same tactic. The “we don’t know” tactic.
“It’s a real mystery why babies are suddenly dying; we should really look into that.”
“It’s a real mystery why healthy adults are suddenly dying; we should really look into that.”
Anyway, I now realise that “Sudden” is part of the obfuscation toolkit. And it works.
Candace doesn’t spend too much time on Tetanus, but she doesn’t need to, she makes the point about necessity very effectively with just a few data points:
Tetanus vaccination began in the US in 1947
That year the US population was 147m
That year there had been 472 Tetanus cases in the entire US (WITHOUT vaccination)
Let’s pause and chew on this for a moment.
That means that there was a 1 in 311,000 chance of getting Tetanus in the US in 1947. Back then you had a 90% chance of dying in you got Tetanus, today it’s a 90% chance of surviving if you get Tetanus. In the vaccine information they gave us back in 1998 (yes, my wife has kept them all!) there is this ominous bit of fear mongering about Tetanus:
Tetanus is a severe, often fatal disease of the nervous system. The person suffers severe painful muscle spasms, convulsions and lockjaw. Even with modern intensive care about 1 in 10 people will die.
Nowhere in the “disinformation sheet” is there ANY mention of your CHANCES of getting it, but if you do get it, they frame it as “even” with the best care in the world 1 in 10 will die, instead of saying that even if you get it, and it’s almost impossible to get it, then 90% survive.
So, the idea underpinning a national vaccination campaign would then be that we need to inject 311,000 with a cocktail of chemicals to eliminate 1 Tetanus case (based on 1947 numbers) and 0.9 deaths (as at 1947) and 0.1 deaths today.
I am going to be pedantic with numbers for a moment.
To prevent 1 death in 1947 you had to inject 345,555 people.
To prevent 1 death today, using the same case ratios even though they have improved dramatically from 1947, you need to vaccinate 3,110,000.
Is this starting to seem absurd to you?
At what point do you simply say NO?
Have I mentioned that Tetanus is NOT infectious, you cannot catch it from someone, so why is it part of a program designed to get to “herd immunity”?
Another point worth mulling over is that a 1 in 311,000 (1947) risk of getting Tetanus is not spread evenly between all 311,000 people. Not everyone of this 311,000 group are going to step on a rusty nail nor are they all going to share a junkies’ needle.
I don’t know what the risk of Tetanus is from needle sharing, but let’s say that it’s 1 in 1,000 needle sharers.
That means that out of that 311,000 random population, let’s assume 1,000 share needles (which is much higher than the actual number, but I’ll use that number here just to keep the numbers simple to make the point), that means there are two groups, one is 310,000 that don’t share needles and their risk of getting Tetanus is ZERO and another group of 1,000 needles sharers and their risk is 1 in 1,000.
You get the point. RISK is a function of RISK FACTORS. If you don’t have those RISK FACTORS or you don’t expect your child to have them either, then the risk to you is effectively and for all intents and purposes ZERO. We should NOT go around injecting ourselves PROPHALACTICALLY against ZERO risks.
That doesn’t make sense to me.
What is the Threshold of Necessity?
Is there even a threshold or has there ever been?
If there was a 1 in 1 chance of dying from something, I’m happy to say that the risks of a chemical intervention that reduces those odds makes absolute sense. You cannot get much worse that 1 in 1.
If there was a 1 in 1 Trillion chance of dying from something, I’m happy to take those chances instead of risking a chemical intervention. Can we all agree that a 1 in 1 Trillion chance is worth taking? Even if you are the most avid vaccination zealot, can we agree that we don’t need to vaccinate anybody against something that has a 1 in 1 Trillion risk? Surely, we can agree to that. If you are a local doctor who is prepared to switch your brain on for a moment, can we agree that a 1 in 1 Trillion risk is not something we need to worry about, or risk an injection to pre-empt?
Ok, so we have our two agreed upon extremes. 1 in 1 (YES vaccinate) and 1 in 1 Trillion (NO don’t vaccinate).
Somewhere along this continuum the average and reasonable person went from a YES to a NO. This is something that you need to think about for yourself and get your own data on, because Vaccine Pharma will NOT tell you the Absolute Risk odds.
So, how to think about it. Here is one way.
The RISK of living in Australia is 1 in 156. There are 25m people and about 160k die each year. That’s nationally 1 in 156. But we know that the risk is heavily concentrated towards the very old. I don’t know the exact numbers but I’m going to use pareto style logic to at least articulate the shape of the argument. I’m going to use 90/10 as my rule.
Let’s say that 90% of the risk of death is in the oldest 10% of the population which is about 73 years old and above.
So, all below 73 have only 10% of the risk of dying FROM ALL THINGS.
That means out of 22.5m (90% of 25m) 16,000 will die (10% of 160k) which equals 1 in 1,406.
Obviously as you get younger these odds exponentially improve.
For the sake of argument, I’m going to say that 1 in 5,000 risk of dying from something is my THRESHOLD OF NECESSITY before I’m prepared to hear arguments about injecting myself and others with any chemical brew. Even then I might decide it is not necessary that the risks and too great. But if I have to pick a number, I’ll go with 1 in 5,000 for now.
There is NOT A SINGLE DISEASE on the vaccination schedule that poses an Absolute Risk below that schedule. If there is, please point me to the numbers so I can eat humble pie and rewrite this post.
This way of thinking is a cornerstone of the 3 legged stool model of deciding whether to vaccinate your child or not.
1. Necessity
2. Safety
3. Effectiveness
If anyone of these legs falls over, then the whole stool falls over and you shouldn’t vaccinate. Understanding the absolute risk of a disease is the cornerstone of coming to terms with the Necessity leg of the stool.
Injecting babies with chemicals to pre-emptively protect them in the very distant future in case they step on a rusty nail is profoundly stupid on the “buyers” part and profoundly evil on the “sellers” part.
Snake oil at its very best.
Is that where all this comes from? Is it the long tail of a Mississippi river snake-oil sales culture?
The CDC claims that vaccination has reduced Tetanus cases by 95% (and death by 99%). Yes, cases and deaths have reduced but I’m not prepared to give any of that credit to vaccination. If you simply look at how people get Tetanus such as stepping on rusty nails and junkies sharing needles, well there are far fewer rusty nails lying around per 100,000 people than in 1947 and there are far fewer people needing to share needles per 100,000, so just on those two variables, they have dramatically improved over the last 70 years, plus better nutrition (which means better immune systems) and better sanitation and better healthcare…basically better EVERYTHING. The sum of all those reasons are why Tetanus cases have dropped significantly. NOT vaccination.
The CDC (and all over sub-agencies of the CDC such as Australian Government Health) crow that Tetanus CASES have dropped by 95% and DEATHS have dropped by 99% and give the majority of the credit, falsely, to vaccination.
Yes, it is true that cases have dropped by 95% but using statistics to lie to the public is one of the oldest tricks. In fact, How to lie with statistics is one of Bill Gates’ favourite books. He is quite open about it.
For cases to drop from 472 pa 70 years ago to about 30 pa (in US) today simply means that Tetanus went from NOT being a threat to the public to NOT being a threat to the public. That’s it.
This is a most wonderful example of the abuse of Relative Risk vs Absolute Risk. They used this same trick in the Covid jab trials, when they said it was 95% effective.
472 to 30 is a 94% drop…sounds great.
But the risk of death has dropped from 1 in 345,555 to 1 in 3,110,000, with that drop being the result of a whole litany of other reasons and NOT vaccination.
I doubt that a reasonable person, knowing the facts, would believe that their baby needs to be injected with aluminium and natural rubber to protect against a 1 in 3,110,000 risk of dying today from Tetanus.
Candace refers to her Patreon account for supporting material to her Parler episodes.
Here are all the supporting references to episode 7:
1. USN News: U.S. Kids More Likely to Die Than Kids in 19 Other Nations
2. NIH: Sudden infant death following hexavalent vaccination: a neuropathologic study
https://pubmed.ncbi.nlm.nih.gov/24083600/
3. A federal court acknowledged that vaccines “causes or substantially contributed to a 2011 SIDS death” they wrote that there was “preponderant evidence supporting that claim. Here is the story of that ruling (Top of page 6)
https://ecf.cofc.uscourts.gov/cgi-bin/show_public_doc?2013vv0611-73-0
4. CDC: Tetanus cases have declined
https://www.cdc.gov/tetanus/surveillance.html
5. CDC: About Tetanus
https://www.cdc.gov/tetanus/about/index.html
6. CDC: Tetanus Symptoms and Complications
https://www.cdc.gov/tetanus/about/symptoms-complications.html
7. Tetanus Fact Sheet
https://www.dshs.texas.gov/IDCU/disease/tetanus/Tetanus-fact-sheet.doc
There are a couple of passages from an Australian by Bran Thomas titled Vaccination Panic in Australia:
A central argument for mass vaccination is that the community benefits from herd immunity. In Australia, there is an aspirational target of having 95% of children fully vaccinated. This is considered more than enough to achieve herd immunity for measles, the most infectious vaccine-preventable disease, and therefore is enough to prevent transmission of all other vaccine-preventable diseases.
Vaccination coverage considerably lower than 95% would be adequate to provide herd immunity for some diseases, for example polio. Then there is tetanus, which is not contagious at all: there is no benefit to an individual due to others having immunity.
I think Brian might believe in some vaccination, but at least he is talking common sense when he states the simple fact that Tetanus is NOT contagious, so what is the point?
So why are there targets for the proportion of children being fully vaccinated — namely having all recommended vaccines at the scheduled times — rather than separate targets for different vaccines? The possibility of having different target vaccination rates for different diseases is never discussed openly by health departments, but the reason is easy to see: it would be an administrative and public relations nightmare. Some parents might seek exemptions for specific vaccines, and record keeping would be more complex. More importantly, though, the vaccination message would be muddled. Rather than saying to parents, “Now’s the time for your child’s MMR, and then it’s time for polio” and so forth, the message might be “It’s really important that your child receives the measles vaccine on schedule, but for tetanus it’s less urgent.”
The bundling of different vaccines into a single concept of vaccination is aided by multivalent vaccines, in which two more vaccines are combined in a single injection, for example measles, mumps and rubella in MMR and diphtheria, pertussis and tetanus in DPT. This means a parent can’t come along and say, “Let’s have measles and whooping cough (pertussis), but postpone the others.”
His point about COMBO vaccines is spot on and rings true to me. It is a CHOICE reducing tool for parents and an EFFICIENCY tool for the public health bureaucracy.
Neither of those two reasons are about your baby’s health.
Let’s move onto sterilization.
This is a weird one for me and forms part of my “pandemic awakening”.
If you had asked me in 2019 what I knew about or thought of “population control” I would have first asked “what do you mean?” and probably settled on saying that the programs around the world are just making contraception pills and condoms more available. That’s it. Giving people around the world access to more CHOICE…and that surely isn’t a bad thing…that would have been the shape of my answer.
And then I read the Fauci book and realised I was living in a fantasy world of prancing unicorns that was entirely disconnected from reality.
How many times have you heard someone say to you “There are too many people on this planet”?
If the man and woman on the street says and believes that do you think there are people higher up that believe it?
Do you think there are people really high up that really believe it?
Do you think there are people really high up that really believe it and really want to do something about it…and are doing it?
Until I read the Fauci book I would have leaned towards NO. Now it’s a clear YES.
Overpopulation is a genocidal idea that is built of sand. The world is just fine with the number of people it currently has and can deal with plenty more. The average calorie intake of the average global citizen is the highest it has ever been, clearly, we can comfortably feed all 9 billion people. Anyway, the facts on this subject are maybe for another post, but for now I am going to state is as simply and categorically as I can.
There are NOT too many people on this planet, and we don’t need to be going around killing people, and the unborn, and even those yet to be conceived, to SAVE THE PLANET.
Here is something short and heterodox on the subject:
Malthus was wrong from the beginning and has been wrong at every turn.
Here is the lovely and very harmless looking Malthusian old lady Jane Goodall (of gorilla fame…look it up) talking about too many humans being the problem. How genocidally sweet.

A wonderful Substack that has emerged in recent times is The Forgotten Side of Medicine by A Midwestern Doctor.
He or she writes in detail about the history of medicine and depopulation.
For example, here is one post with several references to Tetanus vaccination.
The Complete History of Depopulation Vaccines
The Tetanus-Diptheria-Pertussis vaccine has a very questionable past. Due a petty squabble between England and Ireland that originally arose over an English King wanting a divorce, the English treated the Irish terribly. Irish orphanages in multiple cases were used as testing grounds for experimental vaccinations.
In 2014, unmarked mass graves belonging to Irish orphans were discovered. Further research revealed these graves belonged to a group of 2,051 children on which an early and dangerous diphtheria vaccine was covertly tested on in the 1930s. This unethical human experimentation on Irish children (including infants and handicapped children) continued at least through the 1960s and 1970s at Irish care homes, where a separate investigation found early Tetanus, Diptheria and Pertussis vaccinations were covertly tested on these children.
The whole cell pertussis vaccine (given in combination with tetanus and diptheria) developed through these programs was problematic. Physicians at the time observed that sudden infant death syndrome (SIDS) did not exist prior to introduction of the vaccine, and infant death always happened in correlation with vaccination. I have seen a variety of different resources on exact timing of SIDS, but most references state that 90% of SIDS occurs between 2-4 months of age, and the 3 doses of the DTP vaccine are typically given at 2, 4 and 6 months of age.
The evidence that most strongly supports this hypothesis came from the initial COVID lockdowns. Many people in the conventional medical community predicted that infants not coming in for their well child (vaccine) visits would be severely harmed. In contrast, individuals in the vaccine safety movement predicted before the data was even available that this was a once in a lifetime opportunity to see a reduction in SIDS. A reduction in SIDS did occur, alongside an unprecedented decline in premature births (which are also linked to vaccination).
In addition to SIDS, the DTP vaccine was known for causing brain damage, and to some extent is correlated with increasing crime and ADHD rates (both of which are often reflective of brain damage). The brain damage issue was quite common (two children within my extended family for example experienced these complications) and a torrent of lawsuits were filed against the manufacturer in the 1980s. Since the legal cost of these lawsuits exceeded the revenue from vaccination, that litigation situation served as the basis for the creation of National Vaccine Injury Program.
The program was intended to be a compromise between consumer advocates in Congress creating support for parents who were facing unreasonable difficulties in the courts and the manufacturers who needed a way to be able to continue producing vaccines. Fauci played a key role in brokering this deal, and the program rapidly drifted from its original vision to one that protected vaccine manufacturers from all legal liability. This led to a gold rush to add more unsafe vaccines to the vaccine schedule. An explosion of chronic autoimmune and neurologic illnesses (such as autism) followed not long afterwards within the population (the Real Anthony Fauci provides an excellent summary of these changes).
When this article was first written, “Joe” wrote a comment which then got incorporated into the full article. Here is the full comment about his wife’s experience in Kenya:
6 April 2021
My wife is Kenyan and sometime around 15 years ago, when she was still a teenager, she was forced to take one of those “tetanus” vaccines. She and another student who had refused were cornered in a room and forcibly administered the shot. Nearly every one of her school mates whom she is still in touch with have developed some sort of fertility-related problem, and difficulty bringing a baby to full term. My wife herself has had multiple miscarriages. horribly painful and several weeks-long menstrual cycles, sudden death of the baby in the womb, and more. We have one baby who lived. The doctor who delivered her via emergency Csection said he had never seen anything like it....everything was going wrong, the baby stopped developing early on.....our daughter is now 5 and is normal in every way, but it is a miracle.
The girls from her village who were too poor for school fees were spared the vaccine, and they haven’t had any problem conceiving or giving birth.
This horror is still going on in Kenya, now with the Covid shots. We were able to get documentation for most of her family without actually having to get the vaccines, but her sister who was away at boarding school was just forced to get the first Covid shot or she would have been prevented from sitting the national exam. We weren’t able to reach her because she has no phone and I’m not sure what we could have done anyway, because without the exam results you can’t do much of anything in Kenya.
These people who conceived of and are executing these programs are monsters, not human beings. They deserve the death sentence, the same sentence they have administered to millions of unsuspecting, unwilling subjects all throughout the world, and especially in Africa.
And finally, here is an excerpt from The Real Anthony Fauci that goes through some history on vaccines as sterilizing tools and covers the Tetanus campaign in Africa that was laced with a sterilizing agent hCG with anyone being told, least of which the women that were injected.
Sterility Vaccines / Chemical Castration
Gates’s defenders ridicule as “conspiracy theory” the suggestion that Gates, or any reputable public health authority, would use “life-saving vaccines” as a stealth vehicle for surreptitiously rendering women infertile. But one of Gates’s earliest philanthropic undertakings was a 2002 project to administer tetanus vaccines to poor women in fifty-seven countries. For reasons we are about to discover, critics credibly suggest that these vaccines may have been secretly laced with a formula the Rockefeller Foundation developed to sterilize women against their will.
On November 6, 2014, four years after Gates pledged at a TED Talk to use vaccines to lower birth rates, medical researchers and doctors associated with the Kenya Conference of Catholic Bishops (KCCB) and the Kenya Catholic Health Commission accused WHO, UNICEF, and GAVI of secretly conducting a mass sterilization program against Kenyan women, under the veil of eradicating tetanus disease., The Washington Post reported similar charges by the Kenya Catholic Doctors Association (KCDA).
The Catholic doctors became suspicious due to WHO’s glaring departures from the usual tetanus vaccine protocols. Normally a single tetanus vaccine provides a decade of immunity. Since men and women are equally susceptible, both sexes routinely get the vaccine. But WHO instructed Kenyan doctors to give the vaccine in five administrations, six months apart, and only to girls of childbearing years.
“The defense that the WHO intended only to target ‘maternal and neonatal tetanus’ seems odd in view of the fact that males are about as likely as females to be exposed to the bacterium which is found in the soil everywhere there are animals,” observed a 2011 peer-reviewed study of the controversy. The Catholic doctors also noticed other unusual features of the campaign. For starters, WHO suspiciously initiated its jab campaign not from a hospital or medical center or any of the estimated 60 local vaccination facilities, but distributed shots from the luxurious New Stanley Hotel in Nairobi—an exclusive resort out of reach to most physicians or public health officials. At considerable cost, a police escort accompanied the shots to vaccination sites, where police officers strictly supervised their handling by nursing staff and required clinicians to return each empty vial to WHO officials at Nairobi’s only five-star hotel under the watchful eyes of armed officers.
Four years later, in October 2019, the Kenyan Catholic Doctors’ Association accused UNICEF, GAVI, and the WHO of rendering millions of women and girls barren. The doctors had by then produced chemical analyses of vaccines verifying their allegations. Three independent Nairobi accredited biochemistry laboratories tested samples of the WHO tetanus vaccine, finding human chorionic gonadotropin (hCG) where none should be present. In October 2014, Catholic doctors obtained six additional vials and tested them in six accredited laboratories, finding hCG in half of those samples.
In 2019, a group of independent researchers from Kenya and Great Britain led by University of British Columbia neurologist Dr. Christopher Shaw studied the charges and concluded that “the Kenya ‘anti-tetanus’ campaign was reasonably called into question by the Kenya Catholic Doctors Association as a front for population growth reduction.” The medical researchers characterized the WHO program “an ethical breach of the obligation on the side of the WHO to obtain ‘informed consent’ from those Kenyan girls and women.”
Catholic medical personnel made similar accusations about WHO’s tetanus projects in Tanzania, Nicaragua, Mexico, and the Philippines. Following indignant denials of all such accusations, and obligatory denunciations against its accusers, WHO grudgingly admitted it had been developing the sterility vaccines for decades. WHO nevertheless punished the Kenyan doctors and the community officials who reported the spiked vaccine by canceling contracts for future work.
The Sordid History of Sterility Vaccines
It wasn’t the first time that Catholic medical authorities accused the WHO of a stealth sterilization campaign against African women. As early as November 1993, Catholic publications charged that the WHO was spiking tetanus vaccines to neuter dark-skinned women globally with potent abortifacients. WHO denied the explosive charges.
Shaw’s research team showed that WHO and Rockefeller Foundation scientists began research on “anti-fertility” vaccines for “birth-control” as early as 1972, by lacing hCG with tetanus toxoid, which acts as a carrier for the hormone. That year, WHO researchers at a meeting of the US National Academy of Sciences reported their successful creation of a “birth-control” vaccine that diminishes the βhCG essential to a successful pregnancy and causes at least temporary “infertility.” Subsequent experiments proved that repeated doses could extend infertility indefinitely.
By 1976, WHO scientists had successfully conjugated a functional “birth-control” vaccine. The WHO researchers reported triumphantly that their formula could induce “abortions in females already pregnant and/or infertility in recipients not yet impregnated.” They observed that “repeated inoculations prolong infertility.” More recently, in 2017, WHO researchers were working on more potent antifertility vaccines using recombinant DNA. WHO publications explain that the agency’s long-range purpose is to reduce population growth in unstable “less developed countries.”
The Kenyan tetanus campaign occurred shortly after Gates made his pledge of $10 billion to the WHO with the stated purpose of reducing population with “new vaccines.” Perhaps to emphasize his commitment to population control, Gates recruited his most influential vizier, Christopher Elias, as president of Global Development at the Gates Foundation the following year. Prior to that appointment, Dr. Elias was president/CEO of Gates’s nonprofit PATH, which partners with pharmaceutical companies to distribute vaccines to poor countries by persuading rich and poor governments to fork over moolah to multinational drugmakers in which Gates is invested. Elias ran PATH’s innovative “Sayana Press” injectable Depo-Provera project designed to end-run US safety regulations while reducing fertility of Black African women. That brainchild earned Elias the Klaus Schwab Foundation’s Social Entrepreneur of the Year award in 2005. The Gates Foundation provided numerous grants to PATH, including one in November 2020 (after Elias had moved over to BMGF) “to support clinical development of COVID-19 vaccines by Chinese manufacturers.”
Before PATH, Elias had been senior associate in the international Programs Division of the Population Council, with the responsibility of dampening fecundity throughout Southeast Asia. John D. Rockefeller III founded The Population Council in 1952 at a conference he convened for the high priesthood of population control, including the director of the new Planned Parenthood Federation of America and several well-known eugenicists. Lamenting that modern civilization had reduced the operation of natural selection by saving more “weak” lives and enabling them to reproduce, resulting in “a downward trend in … genetic quality,” the group agreed to create an organization devoted to the “reduction of fertility.” While Rockefeller formally launched the Council with a grant of $100,000 and served as the first president, the next two Council presidents were Frederick Osborn and Frank Notestein, both members of the American Eugenics Society. The NIH and USAID were among the “start-up” funders, and US and foreign governments soon became the Council’s largest financial backers.
The Council does research promoting the use of artificial birth control and abortion and biomedical research to discover and develop new contraceptive drugs and technologies. It collaborated with the Ford Foundation and International Planned Parenthood Foundation to develop large-scale IUD programs abroad, despite its own research doctors warning about acute adverse side effects. Later, the Council played a key role in developing the extremely dangerous hormonal contraceptive implant Norplant.
Historian Donald T. Critchlow wrote that the Population Council “cultivated elite connections and avoided public controversy by identifying itself as a neutral, scientific organization.”
The US Agency for International Development (USAID) conducted a decades-long partnership with the Population Council and cultivated long-term alliances with the Rockefeller Foundation and the WHO researching the use of fertility controls to reduce world population, especially in sub- Saharan Africa. By 2014, Gates and Elias had a reliable collaborator at the federal program: USAID Director Rajiv Shah, who had, prior to winning that appointment, worked a decade for the Gates Foundation, running GAVI’s immunization program for African children.
Dr. Shah joined the Gates Foundation in 2001 and oversaw its alliance with the Rockefeller Foundation in launching the Alliance for a Green Revolution in Africa. He directed the International Finance Facility for Immunization. The IFFI is a shady agency that finances Bill Gates’s global vaccine enterprises in developing nations through a diabolically innovative bond issuance scheme that runs up huge debts in poor countries to finance Gates’s self-serving vaccines. Using sleight of hand, IFFI enriches Gates’s pharma partners with Western financial bonds by passing the costs to future generations in poor countries. Shah raised $5 billion through this swindle for GAVI. At USAID, his primary responsibility was reorganizing the agency to reflect its new biosecurity direction under Obama’s 2009 executive order. Shah left USAID to become president of the Rockefeller Foundation in 2017. Shah has deep links to the intelligence agencies and the oil and chemical cartels. Shah serves on both the Trilateral Commission and the Council on Foreign Relations, two globalist organizations that the Rockefeller/Kissinger alliance largely defined. Shah is a board member of the International Rescue Committee, a nonprofit with long-standing CIA ties. In his 1991 book, Covert Network: Progressives, the International Rescue Committee and the CIA, University of Massachusetts economics professor Eric Thomas Chester exposes IRC as a CIA front. Bill Casey, a lifelong spy, who as Ronald Reagan’s CIA Director helped manage the Iran-Contra affair in the 1980s, chaired IRC from 1970 to 1971. IRC operates in forty countries doing “humanitarian aid.” According to its current CEO, David Miliband, the former UK foreign secretary, Shah’s role on the high-level council is to “monitor political and non-health issues related to prevention and preparedness imperatives for a potential epidemic of global proportions.”
In 1974, USAID and WHO collaborated on the creation of a top-secret “Kissinger Report.” Henry Kissinger—whose patron was Nelson Rockefeller and whose career was deeply enmeshed with the Rockefeller Foundation—drafted the classified White Paper, which became official US policy under President Gerald Ford in 1975. That report, known as the US National Security Study Memorandum 200, outlined the geopolitical incentives for reducing population growth in “less developed countries” (LDCs) to near zero by “reducing fertility” so as to safeguard the economic interests of the United States and other industrialized nations in imported mineral resources.
Kissinger observed that the industrialized West was already having to import significant quantities of aluminum, copper, iron, lead, nickel, tin, uranium, zinc, chromium, vanadium, magnesium, phosphorous, potassium, cobalt, manganese, molybdenum, tungsten, titanium, sulphur, nitrogen, petroleum, and natural gas at high cost. The Kissinger Report anticipated rising prices as population growth triggered instability in African nations.
The high-level US government commitment explains the WHO’s monumental commitment to sterility vaccines. Shaw et al. found 150 research publications emanating from WHO on various infertility formulations between 1976 and 2016 with many thousands of citations.
In the years 1993 and 1994, WHO launched antifertility vaccination campaigns in Nicaragua, Mexico, the Philippines, and Kenya in 1995. In each country, WHO and local government clinicians vaccinated women of childbearing age, telling them that the purpose of the WHO immunizations was to “eliminate maternal and neonatal tetanus.”
A subsequent WHO study of birth control policy, Bryant et al., acknowledged that WHO’s family planning “services” had involved routinely deceiving the persons “served” with “sterilization procedures being applied without full consent of the patient.” Similarly, a 1992 study titled “Fertility Regulating Vaccines” published by the UN and WHO Program of Research Training in Human Reproduction, reported “cases of abuse in family planning programs” dating from the 1970s including:
incentives … [Such as] women being sterilized without their knowledge … being enrolled in trials of oral contraceptives or injectables without … consent … [and] not [being] informed of possible side-effects of … the intrauterine device (IUD).
The authors of that WHO report advised their partners against characterizing their work as “anti-fertility measures for population control,” observing that milder descriptions like “family planning” and “planned parenthood” were more palatable for public appetites. Speaking on behalf of the WHO, Bryant et al. admitted, “It is perhaps more conducive to a rights-based approach to implement family planning programs in response to the welfare needs of people and communities rather than in response to international concern for global overpopulation.”
The targeted regions for the WHO tetanus campaigns are principally the same developing nations that the Kissinger Report targeted. For example, a 2015 news release by Associated Press announced “[tetanus] immunization campaigns to take place in Chad, Kenya, and South Sudan by the end of 2015 and contribute toward eliminating [maternal natal tetanus] in Pakistan and Sudan in 2016, saving the lives of countless mothers and their newborn babies.”
The Kenya schedule was identical to the one published for the WHO birth-control conjugate of tetanus toxoid linked to βhCG: five spaced doses of “TT” vaccine at six-month intervals, which, of course, strongly contrasts with the published schedule for authentic tetanus immunization schedules.
Further Reading
HCG Found in WHO Tetanus Vaccine in Kenya Raises Concern in the Developing World“
Baby-Killing Vaccine: Is It Being Stealth Tested?
Even for those of us who knew the system was corrupted the extent of the fraud is mind blowing, almost unbelievable. Thank you so much for the deep dives into this horror.
I appreciate your thorough analysis of the vaccines you used to assume were fine to inject into your children’s bodies. Mary Holland of CHD says vaccine advocates like Dr. Paul Offit are worried that the COVID jab will invite people to question the entire vaccine schedule — just what you’re doing! Hope you enjoy the attached cartoon I did on this subject. https://annecantstandit.substack.com/p/eye-opener?r=7f8gy&s=w&utm_campaign=post&utm_medium=web