



In 1948, a large part of Finland was handed over to Russia, and the Finns living in this area were forced to relocate back into Finland. Some 400,000 of them. This has been described as the greatest proportional ‘forced’ relocation of any people in the history of Europe. How many people outside of Finland know about this?
About two, and I’m one of them. – Dr. Malcolm Kendrick
I spent a year in Finland, in 1992, during our immigration to Australia from Iraq.
I have great memories of Finland, the cold that is so cold that you cannot make a snowball, the snow will simply not melt and stick together. The forests, lakes and saunas everywhere, and the people. There’s a stoicism about that culture that is easily confused for being “cold” or “distant” and a pragmatism about what is rather than what ought to be. A culture born out of living with nature.
For a couple of months we stayed in a tiny town called Hukkala (from memory, population 17 and a dog) about 50 kms from the city of Joensuu which it turns out is in North Karelia (where the forced relocation occurred). The rest of the time we stayed in Lahti, a major city by Finnish standards in the south.
I’ve been back once in 2019, with my daughter for a nostalgia trip. If you ever get the chance to go, I highly recommend it.
Which is why, when I read Malcom Kendrick’s wonderful book on cholesterol, the Finnish story about Karelia especially caught my attention.
Great Cholesterol Con: The Truth about What Really Causes Heart Disease and How to Avoid It
It turns out that the cholesterol story we’ve been sold is not true. It’s an industrially created narrative.
It’s yet one more “Official Story”, although not one covered by Liam Scheff. This time the authority who has written a book, that you and I can understand, is Dr Malcolm Kendrick.
What you need to build trillion dollar industries is: A problem, a cause, a solution.
It needs to be that simple.
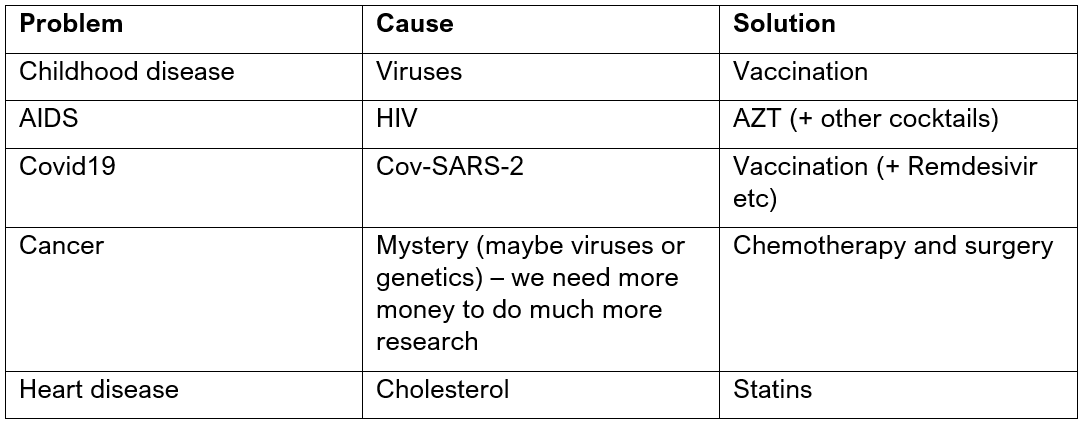
Turns out that cholesterol doesn’t have anything to do with heart disease.
I noticed the video above, where Dr Paul Marik says, “I have to unlearn everything I’ve been taught”, especially because he mentions the statin/cholesterol fraud.
Which reminds me of Dr Robert Yoho’s book, basically making the same point in a different way.

Kendrick wrote a great blog on the subject in March 2022
Pfizer and me – Best Buddies | Dr. Malcolm Kendrick (drmalcolmkendrick.org)
Yes, it’s a little bit funny that Pfizer knew, thirty years ago, that blood clotting and atherosclerosis were intimately connected. They had seen the research. They knew:
‘Important evidence is now emerging that the selective alpha-1 inhibitor, doxazosin, in addition to its beneficial effects on elevated blood pressure and the serum lipid profile, may help to intervene in the evolution of thrombosis, a key component of atherosclerosis.’
In my recent book The Clot Thickens, I said I would put up the Pfizer booklet for all to see. It proved a bit more of a technical challenge than I thought, but here it is. And when people tell me that atherosclerotic cardiovascular disease (ASCVD) is all due to raised cholesterol I can say, not even Pfizer believes that. Not really. Not deep in their hearts …. They have a ghost in the machine that still stalks the corridors of Pfizer HQ. And if it doesn’t, it should.
They knew, oh yes once upon a time, they knew. It’s just not very profitable for them to admit it.
If you know anyone on statins, I would encourage you to buy them the book (it’s not a long read). They are not going to get a straight answer from their cardiologist. They are much more likely to get proper help from an experienced naturopath who has been around for a while, the younger generation seem to have also been captured.
With thanks and gratitude to Malcolm Kendrick. Please buy and share his book.
CHAPTER 10
THE STRESS HYPOTHESIS – DOES IT FIT THE FACTS?
The first task here is to see if the stress hypothesis can explain the huge variations seen in heart disease between different populations – for instance, the twenty-fold difference between Australian aboriginals and the Japanese. In addition, can the stress hypothesis explain why heart disease has waxed and waned so dramatically within populations?
For example, heart disease peaked in the USA more than fifty years ago and has been falling ever since. It is now less than one-third of the level in the 1950s. Following a very similar pattern, heart disease peaked in the UK about thirty years ago, and has been falling steadily ever since. In fact, during the latter half of the 20th century, heart disease has been going down and down in most western countries. In contrast, during the same time period, heart-disease rates have been climbing ever higher in eastern Europe.
In 1968 heart-disease rates in Czechoslovakia and France were the same. Forty years later, the Czechs – and probably the Slovaks too – had 15 times the rate in France. Today, the Ukraine has a rate of heart disease that compares unfavourably with the USA at its very worst; it is about five times the current rate in the UK, and very nearly twenty times the rate in France. But can the entire population of a country be stressed? Have the levels of stress changed dramatically over time? Can these changes, in turn, be related to the rates of heart disease? More importantly, can any of this be proved – in any way?
Some things can never be proved. I cannot go back to the USA in the 1950s and measure HPA-axis dysfunction. Nor can I go back to the UK in the 1970s to do the same thing. What I am going to do, however, is to present a hypothesis about the main ‘stressor’ that causes heart disease – at the level of entire populations. Then I am going to support it using both historical and present data.
This from chapter 9
This ‘three-part’ hormonal system, consisting of the hypothalamus, pituitary gland and adrenal glands, is often referred to as the Hypothalamic-Pituitary-Adrenal axis, or the HPA-axis for short. The HPA-axis is intimately connected to, and intertwined with, the unconscious or ‘autonomic’ nervous system. The autonomic nervous system has two basic divisions: the sympathetic and the parasympathetic systems. Neither of these divisions is under your conscious control – unless you are a Zen master, or something of the sort.
The hypothesis is as follows:
The most deadly long-term stressor that can affect entire populations is something that I define as ‘social dislocation’ – something that as a concept, needs some further explanation. The most straightforward example of social dislocation would be something like ethnic cleansing, whereby a population is forced from their homes at the point of a gun then herded elsewhere. During this process, social and family networks are severely disrupted; family members lose touch – or are killed. Many people find themselves in a different country where they may not speak the language.
Social dislocation need not be as clear-cut as ethnic cleansing, and it can even occur without a population moving at all. Australian Aboriginals, for example, have remained in Australia. However their culture, their lifestyle, their status and their communities have been completely shredded. They now subsist at the bottom of the social hierarchy, with little sense of belonging. They have not physically left their country, but their community has been torn out from under them. Destruction of community can also be seen in other Aboriginal communities, such as the Maoris in New Zealand and Native Americans in the USA and Canada.
On the other hand, social dislocation can be as straightforward as migration to another country. Of course, migration need not be that much of a stressor. A white, Christian, middle-class lecturer moving from Oxford to Harvard is likely to find that most things remain much the same for him or her. And while there may be some sense of temporary disruption, there is unlikely to be any long-term social dislocation. For migration to create a genuine sense of social dislocation, it has to be accompanied by other factors, such as moving to an ‘alien’ culture. This is what happens when, say, an Asian Indian emigrates to a predominantly Christian society such as the UK, USA or Australia. The resultant cultural incompatibility will make it considerably more difficult for such migrants to fit into the surrounding social mores and customs, and gain a sense of being part of a wider community. Indeed, migrants, such as Turks in Germany, or Algerians in France, or Asians in the UK, are often subjected to other major stressors such as racism, lack of job security, language difficulties etc. Their status within the host country is often very low.
The last form of social dislocation I want to look at is when an entire society, or population, is forced to undergo massive change. Most of eastern Europe, for example, has been in a state of turmoil since WWII. Poland, just to take one example, was effectively shifted a hundred miles west, through the re-drawing of its borders. Lithuania, Estonia and Latvia were forced to take in millions of Russian workers that they didn’t want – and who, equally, didn’t want to be in those countries.
In fact, throughout eastern Europe people were forcibly moved between, and within, communities. At the same time, religion was stomped on, churches closed, secret-police organisations set up. All of which would have had a major negative impact on social networks and support. Then, in the late 1980s, communism began to lose its grip, the Wall came down, and the entire Soviet block was plunged into even greater chaos.
That’s the basic description of the main types of social dislocation. So where’s the evidence that it causes heart disease?
SOCIAL DISLOCATION AND HEART DISEASE – AN INTERNATIONAL COMPARISON
Finland – highest rate of heart disease in the 1960s/early 1970s
In the 1960s and early 1970s, Finland had the highest rate of heart disease in the world. Indeed, the country became the epicentre of heart-disease research for a while.
I’d imagine that most people would think of Finland as being a fairly cohesive society, not a country that has been swamped by migrants, or one that has undergone great social upheavals. It seems a tad on the bleak and windswept side to tempt that many people as a dream destination – I’ve been there once and, although I am Scottish, I found it pretty bloody harsh. So what happened to Finland?
Well, after WWII, Russia decided to claim (they called it ‘re-claim’) a large part of Finland called Karelia. This was a time when what Russia wanted, Russia got. The result was that, in 1948, a large part of Finland was handed over to Russia, and the Finns living in this area were forced to relocate back into Finland. Some 400,000 of them. This has been described as the greatest proportional ‘forced’ relocation of any people in the history of Europe.
How many people outside of Finland know about this? About two, and I’m one of them. But the information is all there in black and white. Just type ‘Finland’, ‘Karelia’ and ‘1948’ into a search engine of your choice and bingo! – go read.
To the best of my knowledge no one, at any time, has ever suggested that this massive forced relocation had anything whatsoever to do with the subsequent precipitous rise in heart disease. No one in Finland, no one in the WHO, no one anywhere. This despite the fact that the North Karelia region of Finland – where the majority of those forced out of Russia ended up – had the highest rate of heart disease of any region in Finland.
This, to me, is like finding a whole bunch of people with radiation sickness in and around Hiroshima and failing to recognise that possibly, just possibly, it might have had something to do with the huge atomic bomb that got dropped on it. Hello guys, cause and effect?
The Finns, by the way, have convinced themselves that their superhigh rate of heart disease was mainly due to a bad diet, and that they got rid of heart disease by educating their population on healthy eating, also taking exercise, stopping smoking and suchlike. I am sure that this has had some effect, but they were doing exactly the same things in Sweden, and the rate of heart disease went up there.
Additionally, the main focus of the massive Finnish health intervention trial was done in North Karelia as part of the ‘North Karelia Project’. Yet heart-disease rates fell much more rapidly in the neighbouring region of Kuipio, which was being used as the ‘control’ region, i.e. no health interventions – at all. Of course, this finding has been totally swept under the carpet, but it never fails to amuse me.
To my mind, it is clear why Finland had the highest rate of heart disease in the world in the 1960s and early 1970s. Fifteen or twenty years earlier they had suffered, proportionally, the greatest forced relocation in the history of Europe.
Scotland – highest rate of heart disease in the 1970s/early 1980s
There was a time in the 1970s when Scotland had the highest rate of heart disease in the world. The rate was far worse in the west of Scotland than the east. Everyone points to the predilection of Glaswegians for fried Mars bars and the like, as the reason for their very high rate of heart disease.
What no one points to is the fact that Glasgow is the only major city in Britain to have dramatically shrunk. If I may quote from a website called Glasgow Architecture:
Glasgow Council Housing – History
In 1946, a plan was published by the Clyde Valley Regional Planning Advisory Committee, which had been set up during the war.
It suggested the dispersal of 550,000 Glaswegians into New Towns at East Kilbride, Cumbernauld, Bishopton and Houston. Glasgow at that time had a population of around 1,130,000. [The population is now 675,000 – my note.]
So, the great and wise planners decided to demolish the tenements, and shift 550,000 Glaswegians elsewhere. Of course, this was done after a full consultation process with all 550,000… not.
And what delights awaited the half a million Scots who were relocated from Glasgow during the 1950s and 1960s? Well, here is a description of one of the glorious ‘new towns’ called Cumbernauld. This taken from The Scotsman (a Scottish newspaper):
Criticism of Cumbernauld, created in 1956 for the Glasgow ‘overspill’, usually comes from outsiders. Its stark architecture has few fans and it was described as one of the worst places to live in the UK. The Idler’s Book of Crap Towns said ‘town-planning students visit Cumbernauld to learn what not to do’.
Before that, a business magazine awarded Cumbernauld the Carbuncle Award, bestowed annually on a town deemed to be a blot on the landscape. The town centre was described as ‘a rabbit warren on stilts, a sprawling, angular concrete complex that is soulless, inaccessible, like something from Eastern Europe.’
To be frank, I think they were being polite. I get depressed just driving past.
Now, I have to admit that the tenements of Glasgow were pretty awful. You can read Billy Connolly’s biography to get some feel for just how physically awful they were. There was a sense of community and pride there too, though; people knew each other and looked out for each other (so I am reliably informed). There was a strong sense of ‘belonging’.
However, when the tenements were cleared out the people were moved to some of the most dreary, drab, centrally planned, monstrous high-rise blocks of putrescent concrete ever seen. They still scar the landscape and skyline of Scotland. And they scarred the communities too.
I can assure you that there is nothing in the entire scope of human existence that lays a dead hand upon the soul more effectively than a high-rise flat in Scotland. They are disgustingly ugly, utilitarian and soulless, and they succeeded in obliterating any sense of community, or pride, in those who had the desperate misfortune to inhabit them.
To quote from Glasgow’s official website:
In 1947, a delegation from Glasgow visited Marseilles to see the new ‘tower blocks’ designed by the French architect Le Corbusier, and a high-rise policy was hastily introduced to Glasgow. However, the planners failed to realise that this style was not suitable for all environments and people. Very quickly many high-rise developments deteriorated into dingy, ill-kempt dwellings with resulting problems of social exclusion and despair for the occupants.
As the high-rise flats went up, the old stone tenements came down, victims of the wreckers’ ball in an ill-co-ordinated policy of slum clearance, and damaging local communities in the process. For example, the old Gorbals, captured in the evocative photographs of Oscar Marzaroli, might have been impoverished and rundown, but Marzaroli’s snaps show children playing, neighbours talking on the pavement, and women ‘hingin oot the windae’. For all the material poverty there was a genuine local pride and community spirit.
Contrast the Gorbals ‘New Town’ of the 1960s and 70s, epitomised by the Sir Basil Spence designed Queen Elizabeth flats, an eyesore for miles around until their demolition in the 1990s.
So a big ‘three cheers’ to the socialist planning czars who forced more than half a million people to move. (Sorry, but attempts at social engineering by the self-appointed elite make me very mad indeed.)
Anyway, during the 1950s and 1960s, more than half a million people were forcibly relocated from Glasgow to go and live in a world of soulless concrete, and made-up ‘crap’ towns. In the process, any sense of community spirit was stripped bare leading to ‘social exclusion and despair’.
All of this was followed by a vertiginous rise in the rate of heart disease, which peaked some 15 to 20 years later – and has fallen ever since. Although it has to be said that parts of Glasgow, and the glorious new towns, remain utterly bleak and soulless, and within certain areas the life expectancy is 20 years less than the UK average. That’s right – 20 years.
Roseto – no heart disease at all
Few people have heard of Roseto in Pennsylvania, but it makes an interesting footnote in the history of heart disease. This community was made up almost entirely of Italian immigrants who, in turn, came almost entirely from a Sicilian town called Roseto Valfortore.
So, emigration to a new country followed by a massive rise in heart disease? Ah, no. Emigration followed by a very low rate of heart disease. Why? By way of an answer, I can do no better than to reproduce the entire abstract from a paper called ‘The Roseto effect: a 50-year comparison of mortality rates’:
The Roseto Effect
OBJECTIVES: Earlier studies found striking differences in mortality from myocardial infarction between Roseto, a homogeneous Italian-American community in Pennsylvania, and other nearby towns between 1955 and 1965. These differences disappeared as Roseto became more ‘Americanized’ in the 1960s. The present study extended the comparison over a longer period of time to test the hypothesis that the findings from this period were not due to random fluctuations in small communities.
METHODS. We examined death certificates for Roseto and Bangor from 1935 to 1985. Age-standardized death rates and mortality ratios were computed for each decade.
RESULTS. Rosetans had a lower mortality rate from myocardial infarction over the course of the first 30 years, but it rose to the level of Bangor’s following a period of erosion of traditionally cohesive family and community relationships. This mortality-rate increase involved mainly younger Rosetan men and elderly women.
CONCLUSIONS. The data confirmed the existence of consistent mortality differences between Roseto and Bangor during a time when there were many indicators of greater social solidarity and homogeneity in Roseto
Which goes to show that migration is not necessarily deadly. What kills you is the break-up of the surrounding community.
USA – first country to suffer an epidemic of heart disease
Having mentioned Roseto, I think I should briefly look at the rest of the USA, which was the first country in modern times to suffer an extremely high rate of heart disease.
Although the statistics are not entirely robust, mainly due to the fact that the diagnosis of CHD did not exist until 1948, it is likely that the rate of heart disease rose rapidly during the 1920s and 1930s, peaked some time in the late 1940s and has fallen ever since. I do not think it is any coincidence that this followed a period during which the USA took in more immigrants than any other country in the history of the world. From 1905 to 1914, one million immigrants per year arrived in the USA. Then, in the 1920s, 1930s and 1940s, the rate of heart disease shot up. Since then it has gradually fallen.
This is a pattern that is exactly repeated in other countries that took in huge waves of immigrants. After WWII, Australia and New Zealand took in (proportionally) a huge number of immigrants. The rate of heart disease in both these countries rose rapidly, peaking in the 1970s, before gradually falling.
The Japanese – you see, it isn’t genetics
The Japanese have a very low rate of heart disease (‘It must be genetic…’ Oh do shut up).
However, when the Japanese move to other countries they (usually) lose their protection against heart disease. Most people have put this increase in heart disease down to the fact that when the Japanese migrate they change their super-healthy diet of raw fish, and other such inedible stuff, to fast-food hamburgers – thus causing cholesterol levels to rise. Everyone, it seems, apart from Professor Michael Marmot – the man who runs the Whitehall Study.
Professor Marmot has made a number of studies on the Japanese. He looked at the rising cholesterol levels in Japan and made the following observation in the International Journal of Epidemiology: ‘Considerable increases in total serum cholesterol levels do not offer an explanation of the recent decline in mortality from coronary heart disease in Japan.’ So much, then, for the fast-food conjecture.
In fact, Michael Marmot has long since recognised that the classic risk factors do not remotely explain heart-disease rates, in any population. He was also the first to demonstrate that among the Japanese – as with the Rosetans – retaining your culture is what protects you from heart disease. As he wrote in the American Journal of Epidemiology, as far back as 1976:
To test the hypothesis that social and cultural differences may account for the CHD differences between Japan and the United States, 3,809 Japanese-Americans in California were classified according to the degree to which they retained a traditional Japanese culture. The most traditional group of Japanese-Americans had a CHD prevalence as low as that observed in Japan. The group that was most accultured to Western culture had a three- to five-fold excess in CHD prevalence. This difference in CHD rate between most and least accultured groups could not be accounted for by the differences in the major coronary risk factors.
I have done a bit more hunting on the Japanese, and several other interesting facts emerge. The first is that Japanese Americans have a much higher rate of type II diabetes (adult onset diabetes) than native Japanese. In fact, a study in Brazil found that Japanese migrants had a rate of type II diabetes that was ten times higher than that in Japan. Type II diabetes is a key indicator of HPA-axis dysfunction.
Importantly though, this effect is not seen in Japanese migrants who retain a Japanese lifestyle. In 1996, Dr Boji Huang of the University of Hawaii’s Honolulu Heart Program did a study on Japanese-American men living in Hawaii. He found that ‘A reduced prevalence of diabetes was observed among the men who had retained a more Japanese lifestyle. These findings suggest that living a Japanese lifestyle is associated with a reduced prevalence of diabetes.’
Marmot himself wrote that ‘Japanese culture is characterized by a high degree of social support. There is evidence that this may contribute to the low rate of heart disease in Japan, and among Japanese-Americans who retain their traditional culture.’
On the other hand, studies have shown that ‘non-accultured’ Japanese Americans are much more prone to develop visceral obesity, insulin resistance (diabetes), dyslipidaemia (high VLDL, low HDL) hypertension and coronary heart disease than native Japanese.
At which point it is time to move from the area of hypothesis to the area of hard data.
SOCIAL DISLOCATION AND THE PHYSICAL MARKERS OF HPA-AXIS DYSFUNCTION
While social dislocation cannot be measured, it can be demonstrated that in populations that I would consider to be ‘dislocated’ there are a whole series of measurable metabolic abnormalities to be found. All of which point, in big bright neon lights, straight towards HPA-axis dysfunction.
I could look at many populations, but I will restrict myself to three:
1: Australian Aboriginals
2: Asian Indian emigrants
3: Eastern Europeans
1: Australian Aboriginals
Rapid social and lifestyle changes have been very important in the poor health status of Aboriginals. They are also subject to severe socio-economic discrimination, underemployment, limited education, overcrowding, social depression and severely depressed housing conditions, relative inaccessibility to adequate and nutritious foodstuffs, and limited access to clinical services. Aboriginal people are prone to obesity, hypertension, type-2 diabetes mellitus and cardiovascular diseases - Gracey, M. ‘A pediatrician and his mothers and infants’, Turk J Pediatr, 1997
Australian Aboriginals also suffer very high rates of depression and suicide. They have a rate of type II diabetes (a sure sign of HPA-axis dysfunction) of 21 per cent. This compares with around 3 per cent in the UK. They also show clear signs of excess cortisol secretion. Look under ‘Schmitt, Harrison and Spargo’ for several papers in this area on the pubmed website.
Aboriginals also have high levels of abdominal/visceral obesity, high VLDL levels, low HDL levels and a very high rate of hypertension – often leading to kidney failure. The life expectancy of an Australian aboriginal is 20 years less than that of the surrounding ‘European Australians’.
Of the utmost irony, with regard to Australian Aboriginals, is that the only health intervention that seems to have been put into action is the advice to reduce saturated-fat consumption. And it’s true that their cholesterol levels have dropped a bit. However, in this population a high blood cholesterol – defined as being above 5.5mmol/l – is associated with by far the lowest risk of dying of heart disease. This is one reference that I will provide, as it is a bit difficult to find11.
In fact, in those with high cholesterol levels, the risk of dying of heart disease is 0.29 compared to those with low cholesterol levels – who had a comparative risk of 1. Or, to put this another way, an Australian Aboriginal with a high cholesterol level is more than three times less likely to die of heart disease than an Australian Aboriginal with a low cholesterol level. So, keep up the dietary advice, guys, and see how many more you can kill.
Personally, I don’t think that there can be any doubt that the main cause of heart disease in Australian Aboriginals is an extreme form of social dislocation. They demonstrate every single step from unhealthy stressor, through HPA-axis dysfunction to heart disease. And if you can come up with another reason as to why they have such a high rate of heart disease, then please let me know.
2: Emigrant Asian Indians
It has long been known that Asian Indian emigrants suffer very high rates of heart disease. As I mentioned earlier in the book, this is despite the fact that many of them are vegetarian and rates of smoking in this community are often very low, as are the levels of obesity (at least measured by the body mass index, or BMI).
A study entitled ‘Coronary heart disease and its risk factors in first-generation immigrant Asian Indians to the United States of America’, headed by Dr EA Enas, found that the immigrants had three times the rate of heart disease and eight times the rate of type II diabetes, along with a whole series of other metabolic abnormalities that can be traced straight back to HPA-axis dysfunction:
To conclude, immigrant Asian Indian men to the US have high prevalence of CHD, NIDDM [type II diabetes], low HDL cholesterol levels and hypertriglyceridaemia [high VLDL]. All these have ‘insulin resistance’ as a common pathogenetic mechanism and seem to be the most important risk factors.
In fact, wherever you look, you find the same things in Emigrant Asian Indians. Diabetes, insulin resistance, visceral-fat deposition, high VLDL, low HDL, high Lp(a) et cetera, et cetera. Just to give one last quote from a UK study done by Marmot, Shah and McKeigue and published in The Lancet in 1991:
In comparison with the European group, the South Asian group had a higher prevalence of diabetes (19% vs 4%), higher blood pressures, higher fasting and post-glucose serum insulin concentrations, higher plasma triglyceride, and lower HDL cholesterol concentrations. Mean waist-hip girth ratios and trunk skinfolds were higher in the South Asian than in the European group. Within each ethnic group waist-hip ratio was correlated with glucose intolerance, insulin, blood pressure, and triglyceride. These results confirm the existence of an insulin resistance syndrome, prevalent in South Asian populations and associated with a pronounced tendency to central obesity in this group.
Some researchers have even looked at cortisol levels in Asian emigrants. Unfortunately, most of them persist in doing one measurement at 8 a.m. or 9 a.m. Unsurprisingly, therefore, they keep finding low levels of cortisol. For example, a study carried out in Edinburgh and published May 2006 noted: ‘Cortisol levels are lower in South Asian than in European men resident in the UK. Despite lower cortisol levels in South Asians, the relations between cortisol and cardiovascular risk factors remain strong.’ Bong! Wrong answer. Please go and read Bjorntorp’s work in this area.
Are you convinced yet? Personally, I cannot believe that this research has not been brought together before. To my mind, the true underlying cause of heart disease is ‘stress’ and it’s standing right in front of everyone, jumping up and down, going ‘Hello, look here, it’s me!… Will you please ignore LDL levels… I SAID LOOK OVER HERE! Oh forget it…’
Anyway. It is time to turn to my final population. Which is a big one. It’s eastern Europe.
3: Eastern Europe
I am not going to look at the whole of eastern Europe, you will be pleased to know. Just a few bits. Firstly, I’ll attempt to convey the scale of the problem, which is quite frightening. This from a paper published in the Journal of the American Medical Association in 1998:
Russian life expectancy has fallen sharply in the 1990s, but the impact of the major causes of death on that decline has not been measured. Age-adjusted mortality in Russia rose by almost 33% between 1990 and 1994. During that period, life expectancy for Russian men and women declined dramatically from 63.8 and 74.4 years to 57.7 and 71.2 years respectively… More than 75% of the decline in life expectancy was due to increased mortality rates for ages 25 to 64 years. Increases in cardiovascular mortality accounted for 41.6% of the decline in life expectancy for women and 33.4% for men.
The striking rise in Russian mortality is beyond the peacetime experience of industrialized countries, with a 5 year decline in life expectancy in 4 years time. Many factors appear to be acting simultaneously, including economic and social instability, high rates of tobacco and alcohol consumption, poor nutrition, depression, and deterioration of the health care system. Problems in data quality and reporting appear unable to account for these findings.
Male Russian life expectancy is now 20 years less than that in most of western Europe. And this pattern can be seen across eastern Europe: Latvia, Lithuania, Poland, the Ukraine. You name an eastern European country – after the Wall came down they were all plunged into a health crisis. In truth, Poland seems to be emerging from the other side, and heart-disease rates have been falling for more than ten years. Hopefully, the other countries will soon be following suit.
One group of researchers decided to find out what was behind this unprecedented rise in heart disease. They decided to look at men living in Sweden and Lithuania. What’s more, they decided to measure the differences in ‘psychosocial strain’. I can do no better than to reprint the abstract, because the findings could not be more clear:
Increased psychosocial strain in Lithuanian versus Swedish men (the LiVicordia Study)
OBJECTIVE: Coronary heart disease (CHD) mortality is four times higher in 50-year-old Lithuanian men than in 50-year-old Swedish men. The difference cannot be explained by standard risk factors. The objective of this study was to examine differences in psychosocial risk factors for CHD in the two countries.
METHODS: The LiVicordia study is a cross-sectional survey comparing 150 randomly selected 50-year-old men in each of the two cities: Vilnius, Lithuania, and Linkoping, Sweden. As part of the study, a broad range of psychosocial characteristics, known to predict CHD, were investigated.
RESULTS: In the men from Vilnius compared with those from Linkoping, we found a cluster of psychosocial risk factors for CHD; higher job strain, lower social support at work, lower emotional support, and lower social integration. Vilnius men also showed lower coping, self-esteem, and sense of coherence, higher vital exhaustion, and depression. Quality of life and perceived health were lower and expectations of ill health within 5 to 10 years were higher in Vilnius men. Correlations between measurements on traditional and psychosocial risk factors were few and weak.
CONCLUSIONS: The Vilnius men, representing the population with a four-fold higher CHD mortality, had unfavourable characteristics on a cluster of psychosocial risk factors for CHD in comparison with the Linkoping men. We suggest that this finding may provide a basis for possible new explanations of the differences in CHD mortality between Lithuania and Sweden.
The investigators then went one step further. They measured the levels of cortisol, in response to a standard stress test. Thirty minutes after the stress was applied the change in baseline cortisol level was five times greater in the Swedish men than the Lithuanian men (88.4nmol/1 vs 18.1nmol/1). In their words:
A low peak cortisol response was significantly related to high baseline cortisol, current smoking, and vital exhaustion. The findings suggest a physiological mechanism of chronic psychosocial stress, which may contribute to increased risk for cardiovascular death.
Right is that enough for you? If you don’t believe that social dislocation causes heart disease by now, I’ll never be able to convince you.
Thanks for being here.
Please consider a small paid subscription (donation). The money goes to help covid vaccine injured Australians.
I am always looking for good, personal GMC, covid and childhood vaccination stories. You can write to me privately: unbekoming@outlook.com
If you are Covid vaccine injured, consider the FLCCC Post-Vaccine Treatment
If you want to understand and “see” what baseline human health looks like, watch (and share) this 21 minutes
If you want to help someone, give them a book. Official Stories by Liam Scheff. Point them to a safe chapter, and they will find their way to vaccination.
Here are three eBooks I have produced so far:
FREE eBook: A letter to my two adult kids - Vaccines and the free spike protein


Karelia