


Hepatitis B: The First Vaccine
How to protect your baby from a sexually transmitted disease.


I have two friends who are about to have their first child soon. The day is coming when the doctor is going to “strongly recommend” that their baby be given their first vaccine to protect their new bundle of joy from Hepatitis B.
One of them is now awake to pharma vaccine malfeasance (he read The Real Anthony Fauci…that will do it) but the other isn’t and none of the partners are. This post is for them, and then for anyone else who is about to be faced with the question of whether to start their babies on the long road of chemical injections we call “the vaccine schedule”.
There is something ingenious about framing it as a “schedule”, a bit like buying 10 coffees to get one free and getting a coffee card stamped at each visit. Let’s say that I am worried about whooping cough but not measles, worried about polio but not Hep B, by framing it as a schedule they remove individual agency and all critical thinking about each one of the “coffees”, the goal becomes completing the schedule to get whatever reward is dangled at the end. That reward might be access to childcare or it might just be the “feeling” and the “peace of mind” that my child is now protected against a laundry list of evils.
It's basically a loyalty rewards marketing program.
I’ve had Hep B on my mind for a while, especially in the context of my friends’ births, but this passage recently from Toby Rogers in his letter to Larry Fink nudged me over the line to put this post together:
Vaccine makers were given unlimited liability protection in 1986 via the National Childhood Vaccine Injury Act. With no liability, pharmaceutical companies rushed to add as many vaccines as possible to the childhood schedule without regard for possible harms. While your generation had just a few shots, today women are vaccinated during pregnancy, children are vaccinated on the first day of life (with the incredibly toxic and unnecessary hepatitis B vaccine), and children receive on average 54 shots by the time they reach 18 years of age.
Because of regulatory capture, NONE of the vaccines on the childhood schedule were tested against a saline placebo in a true randomized control trial.
I’m putting together a collection of quality material here for any parent who is prepared to invest 1-2 hours to inform themselves before they inject a cocktail of chemicals into their newborn.
Let’s start off with Candace Owens and Episode Four of here wonderful Shot in The Dark Series on Parler.

This is a great woman doing great work.
Some highlights from this episode are:
Her discussion with the doctor that strongly recommended the Hep B jab for her newborn. Candace simply asked her why she was recommending it and it seemed to be the first time any parent had ever asked that question. The doctors response is interesting in the context of a profession that has been simply brainwashed to parrot the company line.
To the extent that Hep B is a risk, it is a sexually transmitted risk (or needle exchange risk), so why would you be protecting a baby from a sexually transmitted disease? It doesn’t withstand even the slightest questioning and scrutiny.
According to the product insert, they don’t know if the product will work for you and if it does, they don’t know what the “duration of the protective effect” is. I am not making this up.
She makes a very good point about the different disclosures between the clinical trials and the post marketing experience. Basically, what they are saying is that in the clinical trials that they conducted on a small sample of people (without a genuine placebo may I add) they only observed minor adverse reactions (so nothing to worry about). But in the “post marketing”, which means injecting the general population, they have reports of a laundry list of serious adverse reactions, but that “no causal link has been established”. This is the beating heart of the corruption that is the vaccine industry. When we do our trials, we never find anything for you to worry about, but when the general public starts reporting actual real world experiences, you can ignore them because we have made sure that nobody really looks into them carefully enough to “establish a causal link”.
She rightly spends some time on “aluminum adjuvants”.
She highlights the “scripts” that are taught by the CDC to doctors to make sure you get the injection, with “must” sprinkled into many of the scripted answers they are trained to use against the very occasional and curious parent.
She gives you 4 great questions to ask your doctor when they come at you with their rehearsed and scripted medical propaganda.
She talks about the financial incentives that pediatricians have for making sure you take the injection and “stay up to date” with your schedule. These incentives are large enough for many pediatricians to sack you as a patient. I doubt that in Australia this financial incentive model exists, although not sure. Anyway, Australian doctors are so brainwashed and so terrified of stepping outside of the orthodoxy that you don’t really need a financial incentive to nudge them. They simply follow orders.
Here is a list of references that relate to this episode, in case you want to dig deeper:
1. The Insert listed on the FDA website
2. Neo-natal fibroblasts from foreskin are on sale
3. The 15 members of ACIP that make important decisions regarding immunization for our children, per the CDC website
4. British Medical Journal raises questions about the discrepancies in past clinical trials of adjuvant AAHS (Amorphous Aluminum Hydroxyphosphate Sulfate).
5. CDC instructions for how doctors should speak to parents about vaccines, per the CDC Website
6. Critical analysis of aluminum based adjuvants, via the NIH.Gov website.
7. Mice study regarding neurotoxicity of aluminum hydroxide adjuvant particles via the NIH.Gov website.
8. Scientific Study of the "extraordinary high amount" of aluminum content in brain tissue of those with autism spectrum disorder. This study can be found via the NIH.GOV website

Next, I want to spend some time with Kennedy Jr. and his thoughts on Hep B from The Real Anthony Fauci:
Hepatitis B
The conspiracy by GAVI, WHO, and UNICEF to force India to mandate hepatitis B vaccines is yet another illustration of how, under Bill Gates’s hegemony, vaccine industry profits trump public health. The WHO initially recommended hepatitis B vaccination only in countries with high incidence of hepatocellular carcinoma (HCC), the species of liver cancer that the vaccine promises to abolish. Since HCC is rare in India, the country did not qualify under WHO’s initial criteria, which recommended the vaccine only in nations with significant HCC. WHO’s policy meant the vaccine manufacturers would lose a market of 1.3 billion people.
Notwithstanding such concerns about the high costs and meager benefits of the vaccine, Gates, through his surrogates at GAVI, PATH, and WHO successfully arm-twisted the Indian government in 2007–8 into introducing the hepatitis B vaccines.
GAVI pushed WHO to change the official policy to a universal recommendation, meaning that even countries with low disease burdens would be required to vaccinate. GAVI hoped this would reopen the Indian markets. WHO obligingly changed its recommendation to include universal immunization with hepatitis B vaccine for all countries, even those where HCC was not a problem. The Indian government obediently adopted WHO’s recommendation.
Indian academics and public health officials condemned the government’s hepatitis B mandates, citing India’s extremely low burden from HCC. The Indian Cancer Registry (ICMR) shows the incidence of hepatocellular carcinoma due to hepatitis B infection is only 5,000 cases a year. Independent scientists and Indian physicians argued against immunizing 25 million babies each year to theoretically prevent 5,000 cases of HCC. Anticancer vaccines are poor performers, and there is not even meager proof that the vaccine can prevent any cancers. Dr. Jacob M. Puliyel, MD, Chair of the Department of Pediatrics, St. Stephen’s Hospital, Delhi, told me that—even if the vaccine were 100 percent effective—the need to administer 15,000 vaccines to infants to prevent a single death from HCC that might occur decades later “intuitively seems an uneconomic way to spend scarce health resources.”
In a July 17, 1999, commentary published in BMJ, Dr. Puliyel observed that the cheapest Indian hepatitis B vaccine costs 360 rupees ($5.00) for three doses. Dr. Puliyel points out that “a third of [India’s] population earn less than 57 rupees (83p) per capita per month. The main causes of death in India are diarrhea, respiratory infections, and malnutrition.” Puliyel says, “Should immunisation against hepatitis B take priority over provision of clean drinking water?”
The study of Gates’s forced introduction of hepatitis B vaccines in India showed that the vaccine did not reduce hepatitis B. The frequency of chronic carriers (HBsAg positivity) was similar in the unvaccinated as in the vaccinated. The study further suggested that maternal immunity was protecting newborn babies from infection at the time when they are most vulnerable to develop chronic carrier status and HCC, and that the vaccine program reduces this natural immunity. Paradoxically, therefore, there is a substantial likelihood that Gates’s vaccine is increasing the incidence of HCC in the country. These findings demonstrated the absurd futility of hepatitis B vaccination in India. “No matter,” says Puliyel, “Gates’s opinion was the only thing that counted.” WHO stood firm, taking the position that all countries must include hepatitis B vaccine in their immunization program, even if the vaccine was unnecessary.
Frankly I don’t know how you could read that and then still inject your newborn with this junk. Anyway, moving on…
Having listened to Candace I thought I’d have a look at what the Australians say about Hep B. Here is our national schedule. As you can see, Hep B is the very first cab off the rank:
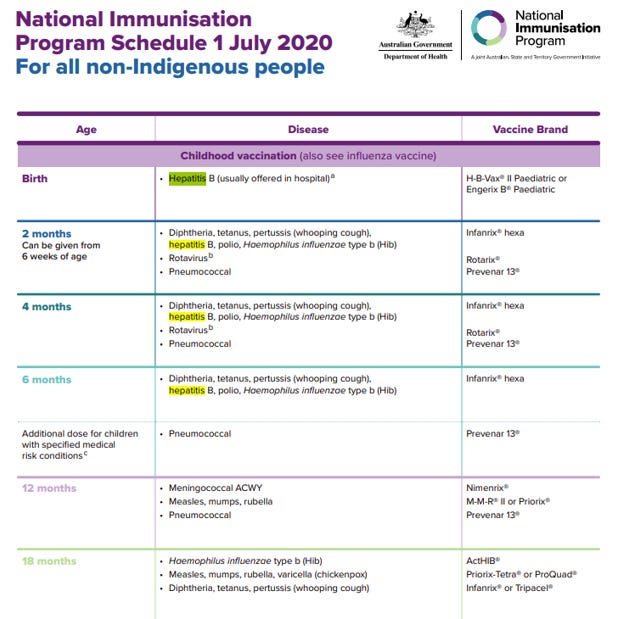
Let’s go deeper into the H-B-VAX® II product information:
What H-B-VAX II is used for
H-B-VAX II is a vaccine used to help prevent hepatitis B. The vaccine can be given to newborns, infants, children, teenagers and adults.
Hepatitis B is an infection of the liver caused by the hepatitis B virus (HBV). It can be caught by coming into contact with an infected person's blood, semen, vaginal secretions, saliva or other body fluids.
So, just to be clear, here is both the government and the product manufacturer telling you that Hep B is transmitted via blood and semen, in other words it’s a sexually transmitted virus, or between junkies sharing needles. Can you remind me again why my baby needs protection from an STD?
By the way, I don’t believe the “saliva” bit. I don’t believe there is quality evidence to support that you can get Hep B from kissing. I’m calling bullshit on that one.
For example, if these infected fluids enter your blood stream through a cut in your skin, you could become infected. Other situations that could lead to infection include:
• being born to a mother who carries the HBV
• sexual contact with someone who is infected
• living in the same house as someone who is infected
• close family contact, for example, sharing razors or toothbrushes
• having a job that involves exposure to human blood or body fluids, for example, some health care workers
• sharing needles for injecting drugs
• travelling to areas where hepatitis B is common
Again, absolutely none of these are a risk factor to a newborn.
People who have hepatitis B may not look or feel sick when infected. In fact, a person could be infected by the virus six weeks to six months before symptoms occur. Some people develop mild, flu-like symptoms. Others may become very ill and extremely tired, develop yellowing of the skin and/or eyes (also called jaundice), dark urine and other symptoms that require hospitalisation.
Most people recover completely from the HBV infection.
Oh, well that’s good to know. So, just in case your newborn miraculously manages to get infected with Hep B, it’s comforting to know that “most recover completely”.
However, there are some people, particularly children, who may not have symptoms but continue to carry the virus in their blood. They are called chronic carriers. These chronic carriers are infectious and can spread the disease to others throughout their lives.
So, let’s get this straight, now you are trying to guilt me into “protecting others” and using a “greater good” argument? I thought this was about protecting my baby. What they are doing is simply creating a narrative of cascading arguments so that if they are forced to retreat from one argument they fall back onto the next. A vacuous charade it most certainly is.
Babies who are infected with the HBV at birth, almost always go on to become chronic carriers. The infection at birth is silent, and the babies appear healthy and continue to remain healthy for many years. However, after 30, 40 or 50 years they can become unwell and develop the symptoms described above.
Here we go again, similar to the HPV scam that injects 11 year old girls against a condition that may occur in your late 50s, here again we have them admitting that you can live a healthy life for 50 years before you “maybe” become unwell. Think about that, are you really going to inject your baby for something that “might” protect them in 50 years?
All chronic carriers run the risk of developing serious liver disease, such as cirrhosis (scarring of the liver) or liver cancer. Vaccination is recommended for adults who are at substantial risk of hepatitis B virus infection. H-B-VAX II works by causing your body to produce its own protection by making disease-fighting substances (antibodies) to fight the HBV. If a vaccinated person comes into contact with HBV, the body is usually ready, and produces antibodies to destroy the virus. However, as with all vaccines, 100% protection against hepatitis B cannot be guaranteed. Because hepatitis B infection can go undetected for a long period of time, it is possible that an individual may already be infected at the time the vaccine is given. The vaccine may not prevent hepatitis B in these individuals.
Some more nuggets from the Australian product information sheet:
Do not have H-B-VAX II if:
• you or your child have an allergy to H-B-VAX II or any of the ingredients listed at the end of this leaflet
• you or your child have an allergy to yeast
Before you or your child are given it
Tell your doctor if:
you or your child have any allergies to any other medicines or any other substances, such as
foods, preservatives, latex rubber or dyes
Can someone please tell me how I would know if my newborn has an allergy to the product that they have never had before, or to the ingredients in the product that I am unaware of and that they have never had before?
Can someone also please tell me how I would know if my newborn has an allergy to latex rubber?
What type of Orwellian, circular logic bullshit is this?
Here is some more detailed product information.
This table about doses caught my eye. Hep B is a three dose vaccine (obviously the problem is so great that it needs three doses!!). This table says that an infant should be given 15 micrograms (3 x 5 µg) vs 30 micrograms for an adult.

Let’s think about this for a moment.
The average weight of a baby girl is 3.4 kg at birth and 4.5 kg after 1 month, and 7.3 kg by 6 months. To keep this simple I’m going to assume an average weight of 5 kgs over that first 6 months. So, 15 micrograms into 5 kgs or 3 micrograms per kilo.
The average weight of an adult woman is about 65 kgs, so 30 micrograms into 65 kgs or 0.46 micrograms per kilo.
So, said another way, a baby girl is getting 6.5 times the per kilo does as an adult woman. Can someone please explain to me how that makes sense?
Or even worse, why is the dose for a baby the same dose as for a 19 year old?
Before we move on, spend some time on pages 6 and 7 reading up on the serious adverse reactions.
Let’s go back to Kennedy Jr. in his discussion on mercury (in the West this seems to have been largely replaced with aluminum). There are several important references to Hep B.
Mercury Rising
Many vaccines shipped to underdeveloped countries— including the hepatitis B, haemophilus influenzae type B, and DTP inoculations—contain bolus doses of the mercury-based preservative and adjuvant thimerosal.
The immunity provisions of the 1986 Vaccine Act gave a blank check to US pharmaceutical companies to promote the most shoddily tested vaccines without consequences or cost. Pharma responded with a gold rush to add new lucrative vaccines to the schedule, and by 1991, mercury exposures to US children from the vaccine preservative thimerosal had more than doubled. Parents, physicians, and researchers blamed a subsequent explosion of neurological and autoimmune disease on thimerosal.
Alarmed at the exploding epidemics of neurodevelopmental, allergic, and autoimmune diseases in children that began in 1986, CDC commenced in 1999 an in- house study of the vast repository of health and vaccination data from the ten largest HMOs stored in the Vaccine Safety Datalink (VSD). A specially assembled CDC research team led by Belgian epidemiologist Thomas Verstraeten compared health outcomes in hundreds of thousands of vaccinated versus unvaccinated children. The raw data from CDC’s 1999 Verstraeten study showed that children who took thimerosal- containing hepatitis B vaccines in their first thirty days suffered an astonishing 1,135 percent higher rate of autism than children who did not. Verstraeten also documented a grim inventory of other neurological injuries including ADD/ADHD, speech and language delays, tics, and sleep disorders in children exposed to thimerosal. Verstraeten reported that these shocking signals prompted him to review, for the first time, the published medical literature, where he confirmed the alarming toxicity of mercury (thimerosal) to cause these injuries was biologically plausible.
Overwhelming science—over 450 studies—by then attested to thimerosal’s devastating toxicity. Because testosterone amplifies the neurotoxicity of the mercury molecule, boys disproportionately suffered reduced IQ and a range of developmental disorders—ADD, ADHD, speech delay, tics, Tourette’s syndrome, narcolepsy, ASD, and autism following exposure to ethylmercury in thimerosal. Numerous studies link thimerosal to miscarriage and Sudden Infant Death. There is simply no study ever published that demonstrates thimerosal’s safety.
In 2017, Robert De Niro and I hosted a packed press conference at the National Press Club in Washington, DC. We offered a $100,000 reward to anyone who could point to such a study. A prestigious group of scientists, including UCLA Fielding School Emeritus Professor of Epidemiology and Statistics Dr. Sander Greenland, toxicologist and past director of the Environmental Toxicology Program at the National Institute of Environmental Health Sciences, Dr. George Lucier, and Dr. Bruce Lanphear of Simon Fraser University and British Columbia Children’s Hospital, agreed to judge the study. There were no takers.
In 2001, the Institute of Medicine recommended thimerosal’s removal from all pediatric vaccines. In accordance with the IOM recommendation, manufacturers removed thimerosal from childhood vaccines—Hib, hepatitis b, and DTP—except multi-dose flu vaccines in the United States beginning in 2001. Japan and the European governments had already dramatically reduced mercury levels in their vaccines as early as 1993.
The European and US bans left Pharma struggling to unload stocks and find new ways to monetize stranded assets —the hundreds of millions in production facilities committed to mercury-based vaccines. Bill Gates came to Pharma’s rescue. Gates helped pharmaceutical companies unload their thimerosal inventories by dumping them in developing countries. Merck, with the help of Bill Gates and GAVI, brokered a deal to donate (dump) 1 million doses of their thimerosal-containing Recombivax HB hepatitis B vaccine to the Millennium Vaccine Initiative to African countries. The White House hailed Gates’s corporate welfare initiative as an “unprecedented level of corporate support” in a press release issued March 3, 2000.
Despite the discontinuance in Western nations, Bill Gates and WHO continue to use their power to force African children to submit to a battery of potentially dangerous mercury-laced pediatric vaccines. Strong evidence suggests that African boys with higher testosterone and chronic vitamin D deficiencies are far more vulnerable to vaccine and thimerosal injury than whites. When it comes to pharma profits, dead and brain-damaged African babies are merely collateral damage.
In 2012, Dr. Fauci waxed philosophical when a reporter asked him to describe an example of one of his useful collaborations with Gates. Perhaps, he speculated, NIAID would work with Gates and GAVI on a project to remove thimerosal from African vaccines. “What is used now is thimerosal, which is frowned upon because of concerns of mercury. So Seth [Berkley, Gates’s GAVI Director] and I were talking about finding a preservative for these multi-dose vials without thimerosal so we no longer would have the baggage associated with it.” By “baggage,” he apparently meant the millions of neurologically injured African children. There is no evidence that this particular collaboration survived its stillbirth as a hypothetical reverie. Eight years later, Africans are still carrying that toxic baggage. It’s a crushing—often mortal—load.
If all of that wasn’t enough, let’s spend some time with Dr. Peter Duesberg in his most wonderful Inventing the AIDS virus.
Part of the Hep B story is the claim that it causes liver cancer. In fact, here in the Australian product pamphlet they say:
All chronic carriers run the risk of developing serious liver disease, such as cirrhosis (scarring of the liver) or liver cancer.
It’s a wonderfully constructed sentence leaving you, the consumer, with the distinct impression that if you get the virus and become a “chronic carrier” then that might well cause liver cancer.
Well, here is Duesberg dispelling as only he can the Hep B virus causing cancer fiction.
THE HEPATITIS B VIRUS-LIVER CANCER HYPOTHESIS
Another product of the War on Cancer emerged during the 1970s, when the virus hunters took up research on liver cancer. This time their sights focused on the hepatitis B virus.
Most people infected by this virus either experience no symptoms at all or experience a temporary liver inflammation, after which their immune systems clear the virus from the body, leaving behind only antibodies against the virus. In a few cases, however - one out of every one thousand infected people in the industrial world and 5 percent of those infected in Asia - hepatitis B can become a chronic infection that neither escalates to kill the patient nor disappears. Instead, it gradually wears away at the victim, constantly damaging the liver while causing on-again, off-again symptoms. People develop chronic hepatitis for understandable reasons, when their immune responses have deteriorated from alcoholism, heroin addiction, or the malnutrition so common in the Third World.
Scientists first noticed an overlap between hepatitis B virus and liver cancer in the 1970s. Nations with high rates of infection also had many cancer patients. Upon closer inspection, some studies revealed that people with chronic virus infections had an enormously higher risk of eventually developing the tumor. In 1978 a paper was published arguing that chronic hepatitis infection directly damaged the liver enough to cause cancer, and another virus-cancer hypothesis was born. No one bothered to point out, however, the complete absence of any evidence for liver cancer being contagious.
As researchers began jumping onto the new bandwagon, they uncovered data that unraveled the virus hypothesis. For one thing, only a tiny fraction of chronic hepatitis cases ever progressed to the cancer, that fraction being much higher among Asians than among Americans. And unlike in the industrial world, where the cultures of drug abuse and prostitution largely transmit the virus, Asians mostly become infected by their mothers around the time of birth. Since liver cancer in the Third World shows up in people between the ages of thirty and sixty years, virologists simply calculated the latent period between infection and cancer as ranging from thirty to sixty years - longer than the life expectancies of many people. No researcher stopped to ask whether other health risks might also endanger the victim during those many decades, obviating the need to blame a virus.
The case for the virus hypothesis degenerated further when most liver cancers were found in patients who had been infected long ago but were not chronic carriers of hepatitis B virus. Rather than continuing as a chronic infection, the virus had been cleared from the body. Hoping to rescue the virus hypothesis, scientists resorted to an old favorite among cancer explanations: Perhaps the tumor could result from cells in which the virus DNA accidentally combines with a specific gene of the cell to produce a cancerous mutation. But follow-up investigations showed that the pieces of viral DNA did not affect any consistent part of the cell's genetic structure and that most of them were biochemically dead and therefore not producing any viral proteins. This implied that such mutations were random, inconsequential accidents. And as with cervical cancer, each liver tumor arose from a single cell at the start, while millions of other cells had been infected with the virus, producing untold numbers of mutant cells. Why did all these other cells remain normal? No answer has been offered. More important, many liver cancer patients have never been infected by hepatitis B at all; in the United States, at least one-quarter of all these tumor patients have never encountered the virus.
Finally, the virus hypothesis has failed miserably when put to the test of Koch's third postulate. Upon injection into chimpanzees, the human hepatitis B virus does infect and inflame liver tissues, but no liver cancer ever appears. The virus, in fact, cannot cause cancer in any animal.
Hepatitis B infections that do not become chronic cannot possibly cause liver cancer. On the other hand, chronic infections might damage the liver enough to promote the tumor. But the more likely explanation for this noninfectious cancer may lie in the health risks, including drug abuse and malnutrition, that allow chronic infections in the first place. Perhaps these risks in themselves cause cancer. Only a small amount of scientific research has examined diet in connection with this cancer-far too little to be sure.
Despite all evidence to the contrary, most scientists still believe wholeheartedly in the hepatitis B-liver cancer hypothesis. It has even become the primary justification for mass immunization programs against the virus in Asian countries, where people inherit the virus at birth and usually suffer no harm. As two biotechnology experts recently put their argument, "While hepatitis B infection may be asymptomatic, chronic carriers have a high risk of developing hepatic [liver] cancer." After three to six decades, that is. Huge government-sponsored vaccination programs are already underway in several Asian nations. Until recently the cost for immunization was $100 per person, now having declined to $38. Given cooperation by the World Health Organization and various governments, such figures can spell enormous income for biotechnology companies, even as they place strains on the economies of nations like Taiwan and Thailand. More than two million people have been vaccinated, and large field trials are being conducted. Since most of these people have been "vaccinated" by natural infection anyway, soldiers in the War on Cancer cannot explain how adding an artificial vaccine could possibly help. Yet they keep marching on.
I want to give the last word to Kennedy Jr. with this lovely bit of trivia that might come in handy during your next Saturday BBQ with family and friends.
What does Hep B and Osama Bin Laden have in common?
The CIA and other intelligence agencies aggressively recruit scientists like Jeremy Farrar, whose research involves postings in foreign countries. Additionally, it uses vaccination drives as a cover for broader strategic actions. Between 2011 and 2014, for example, the CIA used the WHO’s Global Eradication Program to conduct fake polio and Hepatitis B vaccine programs in Pakistan as a way to surreptitiously collect DNA from individuals in its efforts to track down Osama bin Laden.
Great follow up to episode 4 shot in the dark.
Curious for more on this subject, and not wanting to ignore what the current standard advice is, so as not to commit the same error as those who won't listen to 'conspiracy theorists,' I looked up hepatocellular carcinoma on Medscape.
"Hepatocellular carcinoma (HCC) is a primary malignancy of the liver that occurs predominantly in patients with underlying chronic liver disease and cirrhosis. However, up to 25% of patients have no history of cirrhosis or risk factors for it.
"The incidence of HCC has been rising worldwide over the last 20 years [in the face of widespread immunization for decades?!--Fla Mom] and is expected to increase until 2030 in some countries, including the United States.[1] The incidence of HCC is highest in Asia and Africa, where the endemic high prevalence of hepatitis B and hepatitis C strongly predisposes to the development of chronic liver disease and subsequent development of HCC. [but apparently India was a low-incidence country, and it accounts for a large proportion of all Asians, I'd think, so in which Asian countries, exactly, is the incidence highest, I wonder?]
"Current international vaccination strategies for hepatitis B virus (HBV), and advances in the management of hepatitis C virus (HCV) infections, promise to have a major impact on the incidence of HCC, but their benefit will be realized slowly because of the very long latency period—20-30 years—from hepatic damage to HCC development. [lol - *very* slowly, apparently; I wonder if any benefit has been shown in, say, health care workers required to be immunized for these many decades (~40 years ago in my case).]
"Meanwhile, however, there is a growing problem with cirrhosis due to nonalcoholic fatty liver disease (NAFLD), specifically nonalcoholic steatohepatitis (NASH). NASH, which typically develops in the setting of obesity, type 2 diabetes, dyslipidemia, and hypertension, appears to lead the list of risk factors for HCC in the United States.[2, 3] [Doh!] ...
"In general, cirrhosis of any etiology is the major risk factor for HCC.[16, 17] About 80% of patients with newly diagnosed HCC have preexisting cirrhosis. Major causes of cirrhosis in the United States are nonalcoholic fatty liver disease (NAFLD), alcohol abuse, hepatitis C infection, and [bringing up the rear, apparently] hepatitis B infection.[2] ...
"In the analysis of a large managed care database, the incidence of HCC linked to nonalcoholic fatty liver disease rose by 10 times from 0.03-0.46 per 100,000 between the years 1997 and 2005.[21] Currently, HCC non-alcoholic fatty liver disease has the greatest proportion of the burden of the main risk factors for HCC in the United States.[2, 3, 22] ...
"The global prevalence of chronic hepatitis B virus (HBV) infection was estimated to be 296 million persons in 2019[23] ; chronic HBV infection is the most common cause of HCC worldwide [no citation for this comment, I note]. In the United States, about 20% of HCC cases are thought to be related to chronic HBV infection. ...
"It is anticipated that with implementation of worldwide vaccination, the incidence of hepatitis B–related HCC will decrease. In a study from Taiwan, where universal hepatitis B vaccination in newborns and children was instituted in 1984, the average annual incidence of HCC per 100,000 children age 6-14 years declined from 0.70 in 1981-1986 to 0.36 in 1990-1994 (P< 0.01).[24] By the end of 2020, hepatitis B vaccine for infants had been introduced nationwide in 190 countries; in addition,113 countries had introduced one dose of hepatitis B vaccine to newborns within the first 24 hours of life, and the estimated global coverage was 42%, ranging from 6% in the World Health Organization (WHO) African region to 84% in the WHO Western Pacific Region.[25] [It'll be interesting to see what happens to HCC rates in African nations with low HBV vaccine uptake; like having a control group.] ...
"In the United States, liver cancer is the most rapidly increasing cancer in both men and women, with incidence rates more than tripling since 1980; from 2006 to 2015, the rate increased by about 3% per year. ... Liver and intrahepatic bile duct cancers are the fifth most common cause of cancer deaths in men in the US, and the seventh most common in women. ...
"Globally, the incidence of liver cancer among men and women who are younger than 30 years and those aged 30 to 59 years has declined, largely due to national hepatitis B virus (HBV) vaccination programs.[29, 30]
"By racial and ethnic group, rates are highest in Hispanics, followed by Asians/Pacific Islanders, then American Indians/Alaska Natives, blacks, and whites.[28] ...
"[In 2020, t]he incidence was highest in East Asia, at 17.9 per 100,000 population (26.9 in males and 8.9 in females), followed by Micronesia, northern Africa, Southeast Asia, and Melanesia. The incidence was lowest in south-central Asia (3.0 per 100,000) and South America (4.4 per 100,000). By comparison, the incidence rate was 6.9 per 100,00 in northern America and 5.6 per 100,000 in western Europe. Overall, the incidence rate of liver cancer is approximately three times higher in males than in females. Mortality figures mirror the incidence figures.[1] ...
"Steady declines in HCC mortality are predicted for East Asia. In contrast, Northern and Central Europe, North America, and Latin America are showing unfavorable trends.[32] According to an analysis of data from the Global Burden of Disease (GBD) Study, the number of liver cancer cases increased nearly threefold in older men and more than twofold in older women (aged 60 years or more) from 1990 to 2017. The increase consisted mainly of cases secondary to nonalcoholic steatohepatitis (NASH; popularly known as fatty liver disease).[29, 30]" [looking forward to the educational programs on how to prevent and reduce metabolic syndrome, but since educational programs don't make money like vaccines or cancer treatments, I'm not holding my breath.]